Causes of the disease
The exact causes of the formation of esophageal leiomyoma have not been established to date.
Experts put forward only a number of factors that predispose to tumor formation. The following can serve as an impetus for the development of this disease of the esophagus:
- bad habits;
- living in unfavorable environmental conditions;
- genetic predisposition;
- poor nutrition (excessive passion for salted and smoked foods, poor diet, lack of vitamins).
Symptoms and course of the disease
In most cases, leiomyoma does not show any symptoms. However, sometimes the tumor begins to grow and then a number of specific symptoms may appear, such as dysphagia, chest pain, gastrointestinal reflux.
Treatment of the disease
For esophageal leiomyoma, only surgical treatment is performed. These neoplasms are characterized by slow growth, so their removal is indicated only if the functions of the esophagus are impaired. For small tumors, long-term observation with mandatory periodic examination is possible, the purpose of which is to timely establish the indications for surgery. However, early removal of esophageal leiomyomas saves the patient from more complex and extensive surgery in the future.
Most often, surgical removal of leiomyoma is performed by enucleation (husking) of the tumor during thoracotomy. After removal of the tumor formation, the defect in the muscular wall of the esophagus is sutured; for large defects, plastic surgery with a flap of the diaphragm or parietal pleura is possible. Extensive surgery, the purpose of which is to remove part of the esophagus (resection), is performed extremely rarely - in case of large multiple nodes and there is no way to exclude malignancy.
In the postoperative period, the patient is prescribed a diet (mechanically, thermally and chemically gentle dishes). For a long period, drugs from the group of proton pump inhibitors are prescribed, which prevent damage to the mucous membrane of the esophagus by acidic gastric contents. This is especially important if esophageal leiomyoma is accompanied by symptoms of esophagitis.
Examination at Top Assuta
As a rule, leiomyoma is discovered by chance, because it does not have specific manifestations in the first stages. The task of doctors is to objectively assess the picture of the disease and answer the following questions:
- Is it advisable to remove leiomyoma?
- Is the neoplasm prone to malignancy and rapid growth?
- What is the best way to remove it to minimize risks and achieve maximum results?
The Top Assuta diagnostic center has the technical capabilities for 100% accurate diagnostics. The examination is carried out quickly, it is planned in such a way that the patient does not have to queue for diagnosis. Each person arriving from the CIS countries is provided with a Russian-speaking escort.
- Day 1
- Day 2
- Day 3
First day
A consultation is held with the attending physician. It is used for examination and medical history. The oncologist listens to the patient's complaints and specifies the list of studies.
Second day
The following studies are being carried out:
- General blood analysis
- Ultrasound of the esophagus
- Endoscopic examination of the esophagus
- MRI
- Radiography
- Biopsy (performed if cancer is suspected).
The third day
A medical consultation meets, diagnostic data is analyzed, a final diagnosis is made, and a treatment plan is drawn up.
The patient is introduced to this plan in detail and is told what results should be achieved during treatment. For those who want to consult with an Israeli expert, but cannot come to Israel, the Top Assuta clinic offers remote consultation services via Skype. It is budget-friendly, but with the same highly informative diagnostic format. During the consultation, the doctor expresses his opinion on the diagnosis and the effectiveness of therapy in his home country, and also makes recommendations for treatment, which include the most progressive and effective techniques. To get a consultation via Skype, you just need to submit an application on the clinic’s website indicating your diagnosis and contact information, as well as send copies of medical documents.
Prices
| Disease | Approximate price, $ |
| Prices for examinations for stomach cancer | 5 730 |
| Prices for diagnosing Crohn's disease | 3 560 — 4 120 |
| Prices for diagnosing gastrointestinal cancer | 4 700 — 6 200 |
| Prices for hepatitis C diagnostics | 5 700 — 6 300 |
| Prices for treatment of Vater's nipple cancer | 81 600 — 84 620 |
| Prices for colorectal cancer treatment | 66 990 — 75 790 |
| Prices for treatment of pancreatic cancer | 53 890 — 72 590 |
| Prices for treatment of esophageal cancer | 61 010 — 81 010 |
| Prices for treatment of gallbladder cancer | 7 920 — 26 820 |
| Prices for treatment of nonspecific ulcerative colitis | 5 670 |
| Prices for treatment of stomach cancer | 58 820 |
| Prices for diagnosis and treatment of gallstone disease | 9 000 — 11 950 |
| Prices for the treatment of gastroenterological diseases | 4 990 — 8 490 |
| Prices for diagnosing Crohn's disease | 5 730 — 9 590 |
| Prices for treatment of viral hepatitis C and B | 5 380 — 7 580 |
| Prices for treatment of gastrointestinal cancer | 4 700 — 6 200 |
Benefits of treatment at Top Assuta
- Highly accurate and error-free diagnostics
- Highly qualified doctors with extensive practical experience
- High treatment results
- Choosing low-traumatic options for leiomyoma removal
- Affordable prices, no overpayments
Would you like to learn more about how to organize a trip to the clinic? Submit an application on the website and our consultant will provide you with as much information as possible.
- 5
- 4
- 3
- 2
- 1
(1 vote, average: 5 out of 5)
For what reasons does esophageal leiomyoma develop?
The main reason for tumor formation is uncontrolled cell division. This occurs under the influence of various factors of the internal environment. Uncontrolled growth leads to the formation of tumor nodes. There are factors that can trigger such cell growth. These include:
- Chronic diseases of the esophagus and stomach. These include inflammation of the esophagus or esophagitis, the development of reflux and chronic gastritis. Such diseases are a hotbed where inflammation is always present. This is what affects the immune system. Its constant tension leads to loss of control over cell division. This is considered one of the theories for the occurrence of such active growth in a tumor.
- of the bacteria H. pylori in the stomach .
- The presence of other chronic diseases.
- Genetic predisposition. This is due to the fact that a defective gene is transmitted that is responsible for division.
- Presence of a radioactive background.
- Having bad habits such as smoking or alcoholism.
All factors can lead to the development of active growth of muscle cells of the esophagus. Leiomyoma rarely becomes malignant.
Diagnostics
Mostly the tumor looks like a nodular formation with a smooth surface, but it can also consist of several nodules. An experienced endoscopist will detect it by bulging of the wall, if growth is directed into the gastric lumen, and a change in the peristaltic “wave”.
A biopsy of the submucosal node is often inconclusive due to its deep location, so in hardly a third of cases it is possible to judge the true nature of the neoplasm.
High-tech diagnostics - CT and MRI are practically powerless for pathology of the gastric wall; the most effective detection method is endoscopy or endoscopic ultrasonography combined with ultrasound, which allows you to examine the formation from the stomach cavity, determine its boundaries inside the gastric wall, and see the structure and structure of the node.
Symptoms of leiomyoma
Leiomyoma is predominantly a neoplasm of cells with benign characteristics. The appearance of a tumor does not reveal itself in any way, and the first signs may come suddenly. For many years, the disease proceeds secretly and can be detected during an extraordinary diagnosis of the body in a clinic.
The absence of signs is due to the fact that the formation is in a kind of dormant mode and only begins to appear when it increases in size. Like any growing tumor, it creates pressure on nearby internal organs. And when the time comes, leiomyoma is expressed by the following symptoms.
Meal:
- Discomfort when swallowing food, especially hard food. When a person takes food and swallows it, there is a sore throat and pain, like a sore throat.
- Reducing body weight. Leiomyoma begins to grow, blocking the digestive system, and the amount of food entering the body decreases.
- Inability to eat. There comes a time when the tumor completely crushes the organ, and it becomes impossible to eat.
Leiomyoma of the esophagus
Frequent belching occurs during a sharp intake of air and its accumulation in the esophagus. Such conditions cause discomfort and mild pain with an unpleasant odor.
Slow heart rate – there is pressure from expanding tissue caused by progressive leiomyoma on the heart muscle. The frequency of rhythmic oscillations decreases. Also, the heart muscle works intermittently.
Poor supply of oxygen to the lungs:
- Labored breathing. A small-sized neoplasm puts slight pressure on the trachea, often occurring due to the formation of a node in the tracheal area. Compression of the lungs - leiomyoma begins to form, increasing in size, thereby pinching and squeezing the bronchi, which creates difficulty breathing.
- Oxygen starvation occurs when the lungs and trachea are completely compressed and is caused by a neoplasm. Subsequently leads to death without the body being supplied with oxygen.
Hoarse or hoarse voice – fibroids begin to grow and put pressure on the larynx, creating a change in the voice.
One or another single symptom precedes the appearance of a neoplasm.
To simplify the collection of information on population health, a world classification of diseases has been created. The disease has an ICD code of 10 – D13.0 “Benign neoplasm of the esophagus”.
A case of esophageal leiomyosarcoma
The authors presented a case report of esophageal leiomyosarcoma in a 57-year-old man. X-ray and endoscopic examination revealed an exophytic dense tumor with ulceration. The operation was performed: laparothoracocervicotomy, extirpation of the esophagus, esophagogastroplasty with anastomosis on the neck. Histological conclusion: leiomyosarcoma of the esophagus.
The Case of Leiomyosarcoma esophageal
The authors present a description of the case of leiomyosarcoma of the esophagus in men 57 years old. X-ray and endoscopy study revealed exophytic research dense tumor with ulceration. An operation: laparotoracocervicotomy, extirpation of the esophagus, esophagogastroplasty with anastomosis in the neck. Histological conclusion: leiomyosarcoma of the esophagus.
Malignant non-epithelial tumors - sarcomas of the esophagus - are rare and account for no more than 0.5-1% of all malignant neoplasms of this organ [3, 6]. According to V.Kh. Vasilenko et al. (1971), they are almost 200 times less common than cancer. Sarcomas develop mainly in older people, more often in men, and much less often in women. This group of tumors is characterized by the same clinical symptoms (local and general) as with esophageal cancer. Esophageal sarcomas are divided into polypoid and diffuse infiltrating.
Leiomyosarcoma usually develops from the tissue of the walls of large vessels (superior vena cava) containing smooth muscle tissue; most often localized in the lower half of the esophagus. Leiomyosarcoma of the esophagus is extremely rare [2], accounting for about 0.3% of malignant neoplasms of the esophagus [7]. Only isolated observations of this disease have been described in the literature [4, 5, 8]. The surgical approach remains the main one in the absence of signs of dissemination of the process.
We observed a case of esophageal leiomyosarcoma in a 57-year-old man. The patient was admitted with complaints of dysphagia. FGDS revealed a dense infiltrative tumor with ulceration in the esophagus from the mouth to 35 cm along the postero-right wall. X-ray: the esophagus from the tracheal to the supradiaphragmatic segment is sharply dilated, in its lumen there is a tuberous “defect” of filling measuring about 13 by 2.5 cm, with a barium “depot” in the center. The elasticity of the walls of the esophagus in the affected section is limited, and in some areas the walls are rigid. There were no folds of mucous membrane in the affected area.
Rice. 1. X-ray of the esophagus of patient T., 57 years old. The esophagus is dilated and deformed due to a tuberous “defect” of filling, with a barium “depot” in the center. The elasticity of the walls is sharply limited
Rice. 2. X-ray of the esophagus of patient T., 57 years old. In the lumen of the esophagus there are multiple nodes with fairly clear contours. “Niche” on the contour due to ulceration
An operation was performed: laparothoracocervicotomy, extirpation of the esophagus, esophagogastroplasty with anastomosis on the neck. With thoracotomy in the 5th intercostal space on the right, the esophagus is dilated to 8-10 cm. A large exophytic tumor is palpated in the lumen of the esophagus, occupying the upper and middle thirds of the esophagus from the upper thoracic aperture to the supradiaphragmatic region. The case was found resectable. The mediastinal pleura was dissected along the anterior and posterior surfaces of the esophagus, the azygos vein was ligated and resected. The esophagus is mobilized from the esophageal opening of the diaphragm along with paraesophageal tissue and the bifurcation group of lymph nodes to the upper thoracic outlet.
Upper-median laparotomy. Correction of access with four retractors RSK-10. Mobilization of the stomach with ligation of the left gastroepiploic artery, short branches of the splenic artery and right gastric artery, left gastric artery at the origin. Using UO-60 devices, a graft was formed from the greater curvature of the stomach with peritonization of a tantalum suture strip using a continuous suture. Through the posterior mediastinum, the graft was brought into the cervical wound with satisfactory blood flow at the apex of the graft. An end-to-end anastomosis was performed between the proximal part of the graft and the esophageal stump in the cervical wound. A double-lumen nasogastric tube was inserted into the graft.
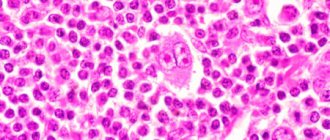
Macro specimen: a soft tissue tumor measuring 12 x 2.5 cm in the shape of an hourglass with clear contours. Histologically: leiomyosarcoma of the esophagus against the background of leiomyoma. There are no metastases along the resection lines and in the lymph nodes and omentum.
Immunohistochemistry: tumor cells are positive for L-smooth muscle actin, about 20% for Ki67, negative for S100, CO 117, CO 34, desmin. Calponin is a uniform positive reaction. Diagnosis: leiomyosarcoma of the esophagus.
R.M. Taziev, D.A. Abdulkhakova, N.V. Balatenko
Kazan State Medical Academy
Republican Clinical Oncology Dispensary of the Ministry of Health of the Republic of Tajikistan
Taziev Ravkat Mingazovich – Doctor of Medical Sciences, Professor of the Department of Oncology and Surgery
Literature:
1. Vasilenko V.Kh., Grebenev A.L., Salman M.M. Diseases of the esophagus. - M.: Medicine, 1971. - 402 p.
2. Davydov M.I., Machaladze Z.O., Polotsky B.E. and others. Mesenchymal tumors of the mediastinum (literature review) // Siberian Journal of Oncology. - 2008. - No. 1 (25). — P. 64-72.
3. Choh JH, Khazei AH, Ihm HJ Leiomyosarcoma of the esophagus: report of a case and review of the literature // J Surg Oncol. - 1986. - No. 32. - P. 223-226.
4. Farkas E., Renyi-Vamos F., Matrai Z. et al. Leiomyosarcoma of the oesophagus: a case report // Magy Seb. — 2006 Dec. — No. 59 (6). - P. 441-4.
5. Hou Y., Wang J., Zhu X et. al. A comparative study of esophageal stromal tumors and smooth muscle tumors // Zhonghua Bing Li Xue Za Zhi. — 2002 Apr. — No. 31 (2). - P. 116-9.
6. Jutley RS, Gray RD, MacKenzie JM, Cockburn JS // A leiomyosarcoma of the oesophagus presenting incidentally without dysphagia. — Eur J Cardiothorac Surg. — 2002 Jan. — No. 21 (1). - P. 127-9.
7. Rocco G., Trastek VF, Deschamps C. et al. Leiomyosarcoma of the esophagus: results of surgical treatment // Ann Thorac Surg/ - 1998 Sep. No. 66 (3). - P. 894-6.
8. Visioli A., Daniel FJ Leiomyosarcoma of the oesophagus: a case report and literature review of leiomyosarcoma // Australas Radiol. — 1997 May. — No. 41 (2). - P. 160-5.