Gastric leiomyoma is absolutely benign in morphological essence, grows very slowly and in most cases does not manifest clinical symptoms. Large nodes can disrupt the normal functioning of the gastrointestinal tract and lead to dangerous complications.
- General information
- Kinds
- Reasons for appearance
- Symptoms
- Diagnostics
- Treatment
- Possible complications
- Prevention
- Forecast
Externally, leiomyoma cannot be distinguished from malignant neoplasms, so it is removed for microscopic and IHC studies, which prove the absence of signs of malignancy.
General information
Leiomyomas develop from cells of the muscular layer of the stomach, which is why their second name is “fibroids.” The tumor develops mainly in older people, but there are known cases of diagnosis of formation in childhood. In the scientific literature of the last century, a more frequent incidence of leiomyoma in women was noted; today, pathology is more often found in men from 40 to 70 years old.
Leiomyoma is a rare pathology and accounts for 3% of all organ neoplasms, but it is also the most common benign gastric tumor - it accounts for almost 45%. Since the process is asymptomatic, in the vast majority of cases, fibroids in the stomach are discovered accidentally during an examination for another reason or at an autopsy. In the last decade, the frequency of pathology has increased; it is believed that the reason for this is the greater availability of medical examinations and mandatory medical examinations.
Differences between uterine leiomyoma and fibroids
Many women are interested in the differences between fibroids, fibroids, fibromyomas and uterine leiomyomas. The medical history of patients often contains both one and the other diagnosis. Essentially, uterine fibroids are the common name for fibroids, fibroids, and leiomyomas. In turn, some differences between leiomyoma, fibroma and fibromyoma still exist and they relate to the structure of the tumors. Leiomyomas contain predominantly smooth muscle cells, whereas fibroids and fibroids are composed of fibrous tissue cells.
Kinds
A generally accepted classification of gastric leiomyoma has not been developed.
Gastric fibroids are usually divided according to the location of the node:
- submucosal or submucosal;
- inside the muscular layer of the stomach - intramural;
- subserous, growing predominantly outward, that is, into the abdominal cavity.
Some experts classify fibroids as:
- internal, growing mainly inside the stomach - endogastric;
- external - with growth directed into the abdominal cavity - exogastric.
By localization in the stomach it is designated as follows: located in the upper third or antrum; in the middle and lower third of the organ.
For gastric fibroids, a typical localization has not been established: approximately a fifth is located in the upper parts, about a third - in the middle part.
Reasons for appearance
The list of reasons for the development of a tumor in the muscular layer of the stomach includes a dozen “general” assumptions, that is, all known risk factors for tumors of any nature are mentioned.
First of all, heredity is suspected - a family history of gastrointestinal neoplasms is assumed without indicating the specific genes “responsible” for initiating the process or hereditary syndromes associated with leiomyoma. The negative impact of radiation, from electromagnetic to radioactive and solar, cannot be ruled out.
Possible factors favoring tumor pathology are immunodeficiency in HIV, as well as hormonal imbalance.
The harmful effects of the environment, unhealthy lifestyle with irregular and unhealthy diet, alcohol abuse and smoking cannot be excluded. And, of course, it was not without the complicity of nervous breakdowns in the initiation of tumor growth.
In fact, none of these reasons has reliable evidence and it would be correct to state the following - the reasons for the development of leiomyomas in the stomach are unknown to science.
Causes
There is currently no clear answer about the reasons for the development of uterine leiomyoma. Experts agree that this disease often develops in women with impaired ovarian function, which is accompanied by excessive production of estrogen. However, in contrast to this theory, there are cases of the development of uterine leiomyoma in patients whose hormonal levels are within normal limits.
In addition, the occurrence of uterine leiomyoma can be provoked by other negative factors:
- surgical termination of pregnancy;
- complicated pregnancy and childbirth;
- endometriosis (adenomyosis) of the uterus;
- inflammatory diseases of the fallopian tubes and ovaries;
- absence of pregnancies and childbirth in women over 30 years of age;
- obesity;
- hereditary predisposition;
- immune and endocrine disorders;
- long-term insolation.
Symptoms
The slow growth and benign course of the myomatous node with high extensibility of the gastric wall in most cases contributes to the absence of complaints of discomfort. It is clear that the severity and range of clinical manifestations are determined by the size and location of the tumor:
- Small or “miniature” leiomyomas do not manifest themselves in any way.
- Large nodes with intracavitary growth can disrupt the evacuation function of the stomach, interfering with the movement of food masses, clinically manifested by belching, vomiting and a feeling of fullness of the stomach after eating.
- Externally located large fibroids, especially on a narrow base - a pedicle, can put pressure on neighboring organs and disrupt their function, as well as twist in the pedicle and simulate an “acute abdomen” clinic with severe pain, vomiting and intoxication syndrome.
The main danger of gastric fibroids is the complicated course of very large nodes, which we will consider further.
Since there is no generally accepted classification of leiomyomas, nodules less than 2 centimeters are considered small, large ones - more than 5 centimeters; the literature contains cases of surgical removal of huge leiomyomas that were masquerading as tumors of the abdominal cavity or ovaries.
Treatment with Mirena coil
The Mirena intrauterine device for uterine leiomyoma is a hormonal IUD of the latest generation and is used for contraception and treatment. Thanks to the main active ingredient - levonorgestrel, the endometrium is thinned, the blood supply to the tumor is reduced, as a result of which many symptoms of uterine leiomyoma disappear.
The use of Mirena for uterine leiomyoma allows you to achieve the following results:
- cessation of intermenstrual bleeding;
- reduction in the volume of menstrual flow;
- elimination of painful sensations in the lower abdomen characteristic of leiomyoma;
- reducing pressure on nearby organs (with subserous leiomyoma);
- improvement of general well-being.
However, the main advantage of the Mirena spiral is that its use helps to reduce the myomatous node itself. Thanks to the normalization of hormonal balance, the tumor loses its stimulus for development. In addition, Mirena helps prevent the development of endometriosis, hyperplastic processes of the endometrium, often accompanying leiomyoma.
Diagnostics
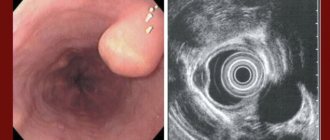
Mostly the tumor looks like a nodular formation with a smooth surface, but it can also consist of several nodules. An experienced endoscopist will detect it by bulging of the wall, if growth is directed into the gastric lumen, and a change in the peristaltic “wave”.
A biopsy of the submucosal node is often inconclusive due to its deep location, so in hardly a third of cases it is possible to judge the true nature of the neoplasm.
High-tech diagnostics - CT and MRI are practically powerless for pathology of the gastric wall; the most effective detection method is endoscopy or endoscopic ultrasonography combined with ultrasound, which allows you to examine the formation from the stomach cavity, determine its boundaries inside the gastric wall, and see the structure and structure of the node.
Treatment
There is no need to remove small tumors that do not bother the patient if there is 100% confidence in their benign nature, but with submucosal growth such confidence is excluded. Benign fibroids and malignant GISTs are visually and morphologically indistinguishable and are differentiated only by immunohistochemical analysis of tumor sections obtained surgically.
The final diagnosis and simultaneous treatment with a diagnosis of gastric leiomyoma consists of their surgical removal. The extent of intervention and access to the organ is determined by the size and location of the tumor, the presence of complications and the patient’s initial health.
In most cases, organ-preserving endoscopic interventions are resorted to, of course, with urgent histological examination during surgery. Laparoscopic resections are quite sufficient and adequate, allowing for rapid recovery of the patient.
In case of a large complicated neoplasm that has caused ulceration of the mucous membrane, perforation of the gastric wall or bleeding, classical operations with dissection of the abdominal wall and gastrectomy are resorted to.
Reviews, prognosis and prevention
According to doctors, if detected early and treated correctly, leiomyoma has a favorable prognosis. Organ-conserving surgeries performed on young women allow them to preserve their reproductive function. Radical surgery may be required only if the fibroids grow rapidly and some other factors, when removal of the uterus becomes inevitable.
In order to prevent the development of this pathology, it is imperative for every woman to regularly visit a gynecologist and perform ultrasound diagnostics, which will allow timely detection of a tumor in the uterus.
The Yusupov Hospital offers a comprehensive examination using modern high-tech equipment. Thanks to the modern equipment of the hospital, the experience and high professionalism of our specialists, we guarantee the most accurate results in the shortest possible time.
Possible complications
Large leiomyomas growing into the stomach cavity disrupt the structural integrity of the mucous membrane, causing its ruptures - erosion and forming ulcers. Ulcerations in clinical manifestations are indistinguishable from a banal ulcer - pain, discomfort, episodes of vomiting, changes in appetite.
And just like ordinary ulcers, they can be complicated by acute or chronic bleeding. Acute gastric bleeding is manifested by vomiting coffee grounds and black stools, decreased vascular pressure up to shock. Chronic blood loss is manifested by anemia syndrome, changes in stool, and weight loss. Insufficient nutrition of leiomyoma leads to the disintegration of its tissues with possible rupture of the gastric wall - perforation and the development of peritonitis.
The complicated course of a benign stomach tumor requires active therapy followed by long-term rehabilitation.
Forecast
Leiomyoma after proper removal does not recur and does not affect the patient’s life expectancy. The literature mentions the possibility of malignancy, which from an oncological point of view is an initially undiagnosed malignant slow-growing GIST; it is because of such cases that gastric leiomyoma must be removed.
A patient with suspected gastric leiomyoma should be operated on by oncological surgeons in a clinic with a powerful diagnostic service and a morphological laboratory focused on oncopathology. During surgery, it is necessary to differentiate a benign process from a malignant one in order to determine the optimal size of removal. The European Clinic is one of the few medical institutions that meet these important requirements for the patient.
Book a consultation 24 hours a day
+7+7+78
Bibliography:
- Gankov V.A., Maslikova S.A., Lazarev A.F., Oskretkov V.I./Surgical tactics for submucosal formations of the esophagus, stomach and duodenum//Bulletin of Med. Sciences No. 2 (10) 2018
- Starkov Yu.G., Solodinina E.N., Novozhilova A.V. /Submucosal neoplasms of the gastrointestinal tract in endoscopic practice// Surgery, 2010; 2.
- Firsov E.I., Vorotyntseva N.S., Novikov M.V. /Comprehensive clinical and radiological diagnosis of benign non-epithelial tumors of the stomach// Kursk scientific-practical. Bulletin "Man and his health", 2009, No. 2.
- Bucber P., Villiger P., Egger JF., et al. /Management of gastrointestinal stromal tumors: from diagnosis to treatment// Swiss. Med. wkly., 2004; 134.
- Greenson JK /Gastrointestinal stromal tumors and other mesenchymal lesions of the gut// Mod. Pathol., 2003; 16(4).
- Nishida T., Blay JY, Hirota S., et al. /The standard diagnosis, treatment, and follow-up of gastrointestinal stromal tumors based on guidelines // Gastric Cancer., 2021 Jan., 19 (1).
A case of ultrasound diagnosis of leiomyoma of the appendix
Ultrasound scanner WS80
An ideal tool for prenatal research.
Unique image quality and a full range of diagnostic programs for an expert assessment of a woman’s health.
Introduction
In recent years, significant progress has been made in ultrasound and differential diagnosis of diseases of the female genital area. With the introduction of transvaginal access, the capabilities of the method in recognizing not only the pathology of the uterus and its appendages, but also other organs located in the lower floors of the abdominal cavity, in particular, the rectum, sigmoid and cecum, have significantly expanded.
As an example illustrating the expansion of indications for transvaginal ultrasound examination in order to detect pathology of the appendix, we present our observation.
Case description
Patient K., 58 years old, complained of almost constant aching pain in the right iliac region, periodically intensifying to acute, paroxysmal pain, weakness, and increased fatigue. Considers himself sick since 1965, when acute pain first appeared in the right iliac region. She was hospitalized with suspected acute appendicitis, but for unknown reasons it was decided to refuse the operation. In subsequent years, repeated attacks of pain in the right iliac fossa resulted in several more emergency hospitalizations. In 1988, she underwent surgery - removal of the right uterine appendages (according to the patient, about a cyst). After the operation, the nature and intensity of the pain did not change, but after repeated examinations, their cause was not established. Over the past year, he has noted an increase in the intensity of pain, a decrease in the “light” intervals between attacks, the appearance of general weakness, and poor health.
In May 1998, to exclude pathology of the large intestine, a colonoscopy was performed, during which a thorough examination of the ileocecal region and the terminal ileum did not reveal any pathology. The expansion of the mouth of the vermiform appendix attracted attention. An attempt to in-depth study of this area led to invagination of the process; during one of the deep antiperistaltic movements, a round, bright crimson formation with a diameter of about 1 cm appeared in the field of view of the endoscope. All subsequent attempts to remove the described formation were unsuccessful, so a targeted biopsy could not be performed. An inpatient examination was recommended, but the patient refused. For re-examination, the patient went to the clinic with the above-described complaints.
Upon examination, the condition is satisfactory, the skin and visible mucous membranes are of normal color and clean. No diagnostically significant deviations from the norm were identified in the heart and lungs. Pulse 81 beats per minute, rhythmic. Blood pressure -140/80 mm Hg. Art. The tongue is moist and covered with a gray coating. The abdomen is soft, of normal shape, moderately painful on palpation in the right iliac region. There was a chair. The liver is not enlarged and not palpable. A survey ultrasound revealed that the liver was not enlarged in size, with smooth contours, the parenchyma had increased echogenicity, and was homogeneous. Intra- and extrahepatic bile ducts and portal vein are not dilated. The gallbladder is large, with homogeneous contents, the walls are not thickened. The pancreas is not enlarged, has increased echogenicity, and is homogeneous. The pancreatic duct is not dilated. In the stomach on an empty stomach there is a lot of mucus, its wall is not thickened (4-5 mm). There were no symptoms of damage to the large intestine. The spleen has an area of 30 square meters. cm, homogeneous. No free fluid is detected in the abdominal cavity. The kidneys are of normal position and size, the collecting systems are not dilated, and no stones are identified. The uterus is small - 3.5 x 2.5 x 3 cm, deviated to the right. The myometrium is homogeneous, the M-echo is linear, 5 mm thick. The ovaries are not visualized. Transvaginal examination in the right iliac region, in the projection of the appendix, reveals a hollow structure with a diameter of 1.3 cm, with hypoechoic walls thickened to 5 mm, presumably the appendix. Adjacent to the described structure is a round formation of reduced echogenicity, with unclear contours, a solid structure, measuring 3.7 x 2.6 cm (Fig. 1).
Rice. 1.
A round formation of reduced echogenicity, with unclear contours, solid structure, measuring 3.7 x 2.6 cm.
A)
A vermiform appendix with a wall thickened to 5 mm and an adjacent periappendicular infiltrate (INF).
b)
The process and infiltrate are circled with the cursor.
Conclusion: suspicion of periappendiceal infiltrate (abscess?). Signs of adhesions in the pelvis. After discussing the results of ultrasound and colonoscopy without other additional examinations, the patient was sent for consultation to the Faculty Surgical Clinic of the Moscow Medical Academy named after I.M. Sechenov, where she was subsequently operated on. During an operation during revision of the cecum, it was revealed that the vermiform appendix can be traced for 2 cm from the dome of the cecum, the remaining sections are represented by a tumor infiltrate measuring 5x3 cm, intimately fused with the body of the uterus and with the posterior parietal peritoneum in the area of passage of the right ureter and iliac vessels . Intraoperative diagnosis: tumor of the appendix with an unknown histological structure, decay and secondary inflammatory changes in both the wall of the appendix and the periappendiceal tissues. With great technical difficulties, a retrograde appendectomy was performed with immersion of the stump of the appendix using purse-string and Z-shaped sutures, partial removal of infiltrated and in places scarred tissue.
Macropreparation: removed appendix with disintegrating tumor tissue, in the center there is purulent-hemorrhagic fluid, 5x3 cm in size, the walls of the appendix are 8-10 mm thick with necrotic mucous and submucosal layers. Histological examination: leiomyoma with fibrosis of the appendix stroma and focal lymphoid accumulations. There are also areas of hemorrhage and necrosis. Pronounced inflammatory infiltration along the tumor capsule from the lumen side. Purulent melting of tumor tissue.
Conclusion
Advances achieved in the field of transabdominal echography for diagnosing intestinal diseases, including acute appendicitis, which is one of the most common causes of surgical intervention, have made it an indispensable instrumental method in the surgical clinic. In the absence of a typical clinic, diagnosing acute appendicitis, primarily in women of childbearing age, is a serious test for the clinician, since many acute and chronic gynecological diseases can simulate an attack of appendicitis. Considerable differential diagnostic difficulties, sometimes errors, arise with chronic appendicitis. In some cases, this leads to unjustified surgical intervention, in others - to an unjustified refusal of surgical assistance.
Leiomyomas, nonepithelial tumors of smooth muscle tissue, are rare (up to 1%) among neoplasms of the gastrointestinal tract. The most common references in the literature are to gastric leiomyomas. Among the available sources, there is no description of leiomyoma of the appendix.
Thus, transabdominal ultrasound in combination with transvaginal scanning makes it possible to accurately determine not only acute or chronic damage to the female genital organs, but also to recognize disease of the vermiform appendix. Therefore, transvaginal ultrasound examination must be included in the complex of diagnostic studies carried out in patients complaining of pain in the lower abdomen, if acute or chronic appendicitis is suspected.
Ultrasound scanner WS80
An ideal tool for prenatal research.
Unique image quality and a full range of diagnostic programs for an expert assessment of a woman’s health.