Live broadcasts on Instagram every Sunday at 12:00
Subscribe so you don't miss out! Subscribe
- home
- general surgery
- Barrett's esophagus
Barrett's esophagus
- This is a precancerous condition that is asymptomatic and is discovered accidentally during a gastroscopic examination.
Columnar epithelium in the esophagus was first described in 1950 by N. Barrett, who mistakenly interpreted this situation as a congenital shortened esophagus. Further in 1953, P. Allison and A. Johnstone established that the described changes relate directly to the mucous membrane of the esophagus, and are a consequence of the replacement of squamous epithelium with columnar epithelium. Then, in 1970, C. Bremner, in scientific work on animals, demonstrated the occurrence of columnar cell metaplasia of the esophageal epithelium in experimentally induced gastroesophageal reflux, proving the acquired nature of such changes and the connection with hiatal hernia or GERD.
The relevance of this problem is that the probability of glandular cancer in patients with columnar cell (intestinal) metaplasia is 0.5-0.8% per year or 5-8% throughout life.
The prevalence of esophageal metaplasia in European residents, according to various sources, ranges from 2% to 5%. At the same time, in the presence of gastroesophageal reflux disease (GERD) with or without hiatal hernia, columnar cell metaplasia of the esophageal mucosa is diagnosed in 10-15% of patients. Adenogenic cancer of the esophagus, which developed against the background of metaplasia, was first described in 1952 by B. Morson and J. Belcher, and in 1975, A. Naef theoretically substantiated the development of adenocarcinoma from metaplastic epithelium of the esophagus. Esophageal adenocarcinoma is a fatal disease with a five-year survival rate of less than 20%, diagnosed in Russia in late stages. Among patients with Barrett's esophagus, the risk of tumor lesions is 30-120 times higher.
In 1983, D. Skinner, using extensive clinical material, proved the presence of a pathogenetic chain: gastroesophageal reflux - columnar cell metaplasia - adenogenic cancer of the esophagus.
The above considerations force us to consider columnar cell metaplasia of the esophageal mucosa as an important surgical problem that requires a thoughtful approach to solving it.
The use of a correct and modern algorithm in the treatment of gastroesophageal reflux disease, which occurs with the development of columnar cell metaplasia of the esophagus, allows, using surgical endoscopic technologies, not only to achieve a significant improvement in the quality of life of patients, but to prevent the development of esophageal adenocarcinoma.
Causes and symptoms of the disease
Barrett's esophagus is a disease that occurs throughout life, often due to the following factors:
- insufficiency of the lower esophageal sphincter, due to which the contents of the stomach (acidic environment) enter the esophagus;
- double reflux - when gastroesophageal reflux disease (GERD) and duodenogastric reflux disease (DGR) develop simultaneously;
- weakened contractile function of the esophagus;
- increased secretion of hydrochloric acid;
- exogenous factors - smoking, dietary errors, excess weight, alcohol abuse, combination chemotherapy.
The most common forms of pathological changes in the mucous membrane of the esophagus, which can lead to BE:
- Dysplasia is a disorder of the normal structure of the mucous membrane, in which cell aging occurs and the tendency to their uncontrolled division increases. This condition is called precancer, since there is a risk of degeneration into oncology, although small. Moderate and severe degrees of dysplasia are distinguished; in severe cases, the risk of developing BE is higher. If provoking factors are excluded, the disease does not progress.
- Metaplasia - in this condition, the normal mucous membrane of the esophagus is replaced by cells unusual for this zone, most often gastric or intestinal. The condition is persistent, it does not disappear even if risk factors are excluded. There is evidence that with a metaplasia length of 3 cm or more, the likelihood of developing a malignant tumor - adenocarcinoma of the esophagus - is higher.
- Erosive form - the presence of erosions and erosive-ulcerative defects (both acute and epithelial) on the mucous membrane of the esophagus in the lower third (usually in the projection of the transition of the esophagus to the stomach).
Main patient complaints and signs of Barrett's esophagus
- pain during swallowing food throughout the esophagus, behind the sternum or in the epigastrium;
- belching with sour contents, especially after eating, heartburn;
- sore throat that occurs after eating, worsens when bending over, hoarseness of voice;
- dysphagia, when the patient complains that it is difficult or painful for him to swallow food, especially solid food;
- nausea and regurgitation after eating, especially when straining or belching;
- thinning of tooth enamel.
You should not ignore the listed symptoms and put off going to the doctor; it is better to prevent the disease and start treatment in the early stages, because the processes occurring at the cellular level are not reversible.
Prognosis for Barrett's metaplasia
Barrett's esophagus is a pre-cancer condition. In approximately 7 patients out of 1000, the disease degenerates into cancer - adenocarcinoma of the esophagus develops. Its mortality rate is close to 85%.
In this regard, predictions are based on the severity of the disease. If, after conservative therapy, pain and heartburn disappear, and the esophageal mucosa is slightly changed, then the prognosis will be favorable. But in the future the patient must undergo follow-up examinations.
With significant damage to the esophagus and progression of the disease, the prognosis is not very good. In this case, the clinical picture of Barrett's esophagus may indicate the beginning of the development of a cancerous tumor of the esophagus.
Don't wait for the disease to take root; don't give cancer a chance to exist. Contact the clinic if there is the slightest change in your health. Assuta doctors will select an individual treatment program for you as soon as possible.
Diagnosis of Barrett's esophagus
The main and most effective method for diagnosing Barrett's syndrome is endoscopic. Its purpose is to obtain biopsy material. In this case, the morphological study is aimed at:
- confirmation of metaplasia of the esophageal mucosa;
- detection of dysplasia;
- detection of malignant cells, most often adenocarcinoma.
To determine more precise boundaries of the changed mucosa during endoscopic examination, chromoscopy is used; this is the coloring of the mucosa. Lugol's solution is usually used; if you are allergic to iodine, use methylene blue or acetic acid.
Treatment of Barrett's esophagus
The following treatment methods for Barrett's esophagus are used:
- Medication . Conducted by gastroenterologists. Antacids that reduce acidity, prokinetics that stimulate motility and the movement of food through the gastrointestinal tract, and proton pump inhibitors are often prescribed.
- Endoscopic . And here the endoscopist has a large choice, it all depends on the volume of the lesion, the severity of dysplasia, the depth of invasion (penetration) and other factors.
- argon plasma coagulation;
- endoscopic resection (dissection) of the mucous membrane;
- endoscopic ablation of the esophageal epithelium with a bipolar electrode;
- photodynamic therapy;
- cryodestruction;
- laser ablation.
- Surgical . To prevent the development of Barrett's esophagus, a Nissen fundoplication is performed. The essence of the operation is that a cuff is made around the esophagus from the bottom of the stomach, which should prevent the reflux of stomach contents into the esophagus.
Another commonly used and very radical method is removal of the lower part of the esophagus.
3.Diagnosis of the disease
Because Barrett's esophagus itself almost never has specific symptoms, it is diagnosed by upper endoscopy and biopsy.
Such an examination is recommended for people who have several
risk factors for developing Barrett's esophagus
- age over 50 years, male gender, presence of a hiatal hernia, long-standing GERD, excess weight.
During endoscopy
The gastroenterologist inserts a long, thin tube with a camera and a light source at the end into the esophagus, examining it from the inside.
You may feel a little uncomfortable during the endoscopy, but it is not painful. When examining the esophagus, the doctor can immediately notice Barrett's esophagus - it is simply visible through the camera. But an accurate diagnosis requires a biopsy
- the doctor will take a small tissue sample, which is then examined under a microscope to confirm the diagnosis.
The tissue sample taken during the biopsy is also analyzed for the presence of precancerous cells or cancer. If the biopsy confirms Barrett's esophagus, another endoscopy with biopsy may be needed to examine more tissue for early signs of cancer. Such examinations will need to be carried out regularly so as not to miss dangerous oncology.
About our clinic Chistye Prudy metro station Medintercom page!
Prevention
There is no specific prevention for Barrett's syndrome.
Timely diagnosis and treatment of gastroesophageal reflux disease, regular and timely visits to a gastroenterologist, examinations and consistent follow-up help prevent its development.
- For dysplasia of the esophageal mucosa, FGDS control with biopsy is required once every 6 months.
- For metaplasia - FGDS control once a year.
After effective conservative and surgical treatment of Barrett's esophagus, all patients should undergo annual endoscopic examination with epithelial biopsy.
Answers to questions from patients with Barrett's esophagus
Can Barrett's esophagus be cured?
Barrett's esophagus is a precancerous condition; if a patient with such a diagnosis has completed the necessary course of treatment, regularly visits a doctor to monitor the situation, and follows all his recommendations, then the likelihood of a cure is very high. This disease, especially in the early stages, responds well to treatment, provided that it is prescribed individually by a competent specialist and is carried out comprehensively. The complex must include all the necessary methods - medication, dietary, endoscopic and surgical. Thus, to completely cure Barrett's esophagus, the joint efforts of the treating physician and the patient are necessary.
How to treat Barrett's esophagus?
In the treatment of Barrett's esophagus, the most important factor is the timely detection of pathology. If the patient undergoes regular examinations, the doctor will be able to detect the disease at an early stage. After effective treatment, the risk of possible malignant cell degeneration will be virtually eliminated.
Treatment is carried out comprehensively and, depending on the specific situation, includes both surgical and conservative methods. The therapeutic program is compiled individually for each patient, taking into account the characteristics of his body and clinical picture. As a result, the risk of further development of pathology and complications that are dangerous to the patient’s life is eliminated, his well-being improves, and his quality of life increases.
If the situation allows only conservative treatment to be prescribed, the patient must be prepared to carefully follow the prescribed medication regimen for a long time (from 3 months to 2 years). In addition, for the success of treatment, a certain correction of the patient’s diet and lifestyle will be required - immunity-strengthening procedures, reasonable dosing of work and rest, weight loss, giving up bad habits (alcohol, smoking, chocolate, soda, tea, coffee).
Many patients, on the recommendation of a doctor, immediately undergo a session of radiofrequency ablation (RFA) of the esophageal mucosa, during which dosed destruction of the altered mucosa is carried out during gastroscopy. As a result of this procedure, the metaplastic epithelium is replaced by normal mucosa. The duration of conservative drug treatment is shortened several times.
If the disease has developed against the background of hiatal hernia and has already entered a stage requiring the use of surgical treatment methods, our clinic uses laparoscopic methods, which are not only effective, but cause a minimum of trauma, and therefore are quite easily tolerated by the patient.
The goal of a complex of surgical and conservative methods is to minimize the risk of cancer and restore the mucous membrane of the esophagus. Also, surgical treatment is prescribed if conservative treatment does not bring the expected results.
How long do people live with Barrett's esophagus?
If treatment is successful, which is most of the time, patients diagnosed with Barrett's esophagus live normal lives.
That is why it is important to identify the disease at an early stage and follow all the recommendations of your doctor. It is not the syndrome itself that is life-threatening, but its complications. Unfortunately, the number of patients with esophageal cancer increases every year. Treatment of esophageal cancer is only surgical and is accompanied by a long and very voluminous surgical intervention with removal of the entire esophagus and plastic surgery with the stomach.
How often does Barrett's esophagus develop into cancer?
Barrett's esophagus differs from ordinary chronic diseases in that the degeneration of cells can become malignant at any time. A seemingly calm disease can suddenly turn into esophageal cancer. Moreover, the oncological process is characterized by rapid development.
Currently, world medicine is noticing a significant increase in the number of patients suffering from esophageal cancer, which is a consequence of advanced Barrett's esophagus. The probability that this syndrome will develop into cancer, according to the World Health Organization, varies in different countries, from 0.5% to 10%. Considering that in our country people tend to pay insufficient attention to their health and attribute alarming symptoms to malaise, the likelihood that the disease will be diagnosed in the later stages and the process of cell degeneration will take on a malignant nature is inclined towards higher numbers.
Therefore, at the slightest suspicion of Barrett's esophagus disease, it is necessary to consult a highly qualified specialist. You can also always write to my personal email: [email protected]
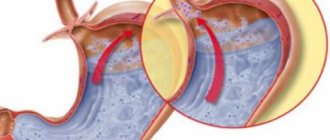
Localization of Barrett's esophagus in the gastroesophageal junction
Visual picture during endoscopy, variants of the mucosa in Barrett's esophagus
Visual image during endoscopy, length of mucosal lesion in Barrett's esophagus