Despite the fact that the length of the small intestine makes up 80% of the entire gastrointestinal tract, the proportion of malignant tumors of this localization does not exceed 1% of the total number of cases of cancer of the digestive tract. The rarity of this disease is explained by the rapid passage of the bolus of food through the small intestine. This reduces the time it is exposed to food carcinogens.
Our expert in this field:
Ryabov Konstantin Yurievich
Chief surgeon, oncologist, endoscopist
Call the doctor
Adenocarcinoma is the most common of all histological types. Carcinoid and leiomyosarcoma are less commonly diagnosed. In children, the main tumor of the small intestine is lymphoma.
Causes of small intestine cancer
Small intestine cancer is a malignant neoplasm of the small intestine: duodenum, jejunum or ileum. In most cases, small intestinal cancer develops against the background of chronic enzymatic or inflammatory diseases of the digestive system:
- Peptic ulcer;
- Celiac disease;
- Duodenitis;
- Enterita;
- Diverticulitis;
- Nonspecific ulcerative colitis;
- Crohn's disease.
Benign epithelial neoplasms of the intestine can transform into a cancerous tumor. Doctors explain the predominant damage to the duodenum by the irritating effect of bile and pancreatic juice on the initial part of the small intestine, its active contact with carcinogens that enter the digestive tract with food.
Increased risk factors for developing small intestinal cancer are sporadic or familial adenomatous polyposis. The likelihood of developing small intestinal cancer is higher for people exposed to radiation or suffering from alcohol addiction, smokers, people whose diet is dominated by canned foods, animal fats, and fried foods. There is a relationship between colon cancer and malignant neoplasms of the small intestine.
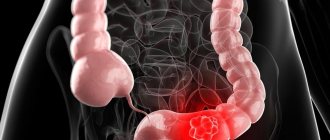
How does bowel cancer develop?
Oncological diseases of the intestine are malignant tumors that develop in the mucous membrane, after which they grow into the thickness of the tissue and give metastases. The reasons for their development can be different - poor nutrition, bad habits, genetic predisposition to cancer, concomitant pathologies, etc.
The neoplasm can affect any part of the gastrointestinal tract and have a different clinical course, which determines the symptoms of the disease.
The highest risk of developing colon cancer develops in adults after 40 years of age, and the peak incidence occurs at 65-70 years of age.
Both sexes have the same risk of getting colorectal cancer, but men are most often diagnosed with colon cancer, and women are most often diagnosed with colorectal cancer. The main danger of the disease is that in the early stages the disease is practically asymptomatic, and it is extremely difficult to recognize it. Once the tumor grows, it becomes more difficult to get rid of it, and the prognosis for patients worsens sharply.
Types of small intestinal cancer
Depending on the nature of the growth of tumor tissue, oncologists distinguish exophytic and endophytic cancer of the small intestine. Exophytic neoplasms grow into the intestinal lumen, causing its narrowing and the development of intestinal obstruction. Outwardly, they resemble cauliflower or a polyp. Endophytic forms of tumors infiltrate the wall of the small intestine in depth. They are accompanied by intestinal bleeding, perforation and peritonitis.
According to the histological structure, malignant neoplasms of the small intestine are most often represented by adenocarcinoma. Less common are sarcomas, carcinoid, and lymphoma of the small intestine.
Symptoms and signs of small intestine cancer
Small intestinal cancer is characterized by polymorphism of manifestations. This is due to the variability of localization, histological structure and size of the tumor. In the initial stages of the disease, patients present the following complaints:
- Periodically recurring cramping pain in the abdomen;
- Stool instability (diarrhea alternates with constipation);
- Nausea and vomiting;
- Flatulence.
If the tumor process progresses, intoxication and weight loss are noted. When a malignant tumor of the small intestine is destroyed, symptoms of intestinal bleeding and perforation of the intestinal wall occur. The contents of the intestine enter the abdominal cavity and lead to peritonitis. Exophytic growth of tumors may be accompanied by symptoms of obstructive intestinal obstruction. If the neoplasm compresses neighboring organs, intestinal ischemia, pancreatitis, jaundice, and ascites develop.
Sometimes the tumor fusions with the bladder, adjacent intestinal loops, large intestine, and omentum to form a single, sedentary conglomerate. When ulceration and decay of small intestinal cancer occurs, intestinal fistulas occur.
Clinical manifestations of ileal cancer develop gradually. The first symptoms are dyspeptic symptoms:
- Nausea;
- Vomit;
- Violation;
- Motor skills;
- Severe spasmodic colic.
Patients quickly experience a decrease in appetite, an aversion to food, and a decrease in body weight. With multiple tumors, intestinal obstruction occurs. It is characterized by abdominal pain, vomiting first of gastric and then intestinal contents, bloating, dry skin and dehydration. With sarcomas of the small intestine, intestinal bleeding is often observed.
Prognosis and prevention
Adenocarcinomas
For a disease such as small bowel cancer, the prognosis for overall five-year survival for resectable adenocarcinoma is 20%.
The five-year survival rate for small bowel adenocarcinoma by stage is as follows:
- Stage I - 70%
- Stage II - 55%
- Stage III - 30%
- Stage IV - 5-10%
A study comparing outcomes for 2,123 patients with small bowel adenocarcinoma and 248,862 patients with colorectal cancer found that the prognosis for small bowel adenocarcinoma is worse than for colorectal cancer, and only surgery improves survival.
Sarcomas
The five-year survival rate for resectable leiomyosarcoma, the most common primary sarcoma, is approximately 50%. For a disease such as sarcomatous tumor of the small intestine, the prognosis improves if negative surgical margins are noted during surgery.
Symptoms of duodenal cancer
The most characteristic and first symptom of duodenal cancer is pain. In the early stages of the disease, pain syndrome involves the nerve elements of the intestinal wall in the pathological process. During this period, the pain is constant, aching, and is not associated with food intake. When the process is locally widespread and the cancer tumor grows into the mesentery of the colon and small intestine, the pancreas, the pain becomes burning. Their intensity and duration increase, and a constant feeling of heaviness appears in the epigastric region.
The development of obstruction is manifested by increasing signs of narrowing of the duodenum. Pain from duodenal cancer radiates to the back. This is due to the common innervation of the duodenum with the pancreas, pylorus, liver and gall bladder, and bile ducts. Small bowel high obstruction may develop when small bowel carcinoid spreads to the mesentery. With exophytic growth, cancerous tumors often undergo decay. In this case, the first sign of the disease may be intraintestinal bleeding.
Cancer of the major duodenal papilla (ICD-10 code C24) causes increased pressure in the biliary zone and the development of obstructive jaundice. Small intestinal carcinoid is characterized by the development of paraneoplastic syndromes that are associated with the production of hormones. Their symptoms are hot flashes, arrhythmias and bronchospasm.
The first symptom of a malignant tumor of the major duodenal papilla is often obstructive jaundice, which occurs against the background of somatic well-being. Initially, the jaundice is intermittent. Normalization of biochemical blood parameters is due to a decrease in edema in the area of the stenotic bile duct. As cancer of the papilla of Vater progresses, jaundice becomes more persistent. After intense pain, accompanied by chills and heavy sweats, patients' skin color changes. Patients complain of severe itching. The transient nature of jaundice in the later stages of the disease is due to the disintegration of cancer of the major duodenal papilla, which is accompanied by a temporary restoration of the patency of the bile duct.
When palpating the abdomen, doctors determine an enlarged liver. In 60% of patients, an enlarged gallbladder is felt under the lower edge of the liver. With prolonged obstruction of the biliary tract, liver cirrhosis and chronic pancreatitis occur. If cancer of the major duodenal papilla grows into the intestinal wall, bleeding may occur with the subsequent disintegration of the tumor. With regional metastasis, the pain syndrome changes.
A characteristic feature of cancer of the major duodenal papilla is early weight loss. The reason for weight loss is the narrowing or blocking of the lumen of the pancreatic ducts, due to which the enzymes that are so necessary for the breakdown of fats and proteins cease to flow into the digestive tract. Weight loss and vitamin deficiency cause muscle weakness.
Patients with cancer of the major duodenal papilla often experience diarrhea. They are accompanied by bloating and abdominal pain. The feces are clayey-gray and foul-smelling. In advanced cases, fatty stool may be detected. When regional metastases appear, the nature of the pain syndrome changes. In the later stages, depletion and dysfunction of organs that are affected by distant metastases are determined.
Diagnosis of small intestine cancer
For a malignant tumor of the duodenum, doctors at the Yusupov Hospital perform fibrogastroduodenoscopy and contrast fluoroscopy. Colonoscopy and irrigoscopy are informative for diagnosing cancer of the terminal ileum. Barium passage X-ray allows you to identify obstacles to the advancement of the contrast agent, areas of narrowing and suprastenotic expansion of the intestine. During an endoscopic examination, the doctor performs a biopsy for subsequent morphological verification of the diagnosis. In cases that are difficult to diagnose, selective angiography of the abdominal cavity is performed.
In order to identify metastases and germination of small intestinal cancer into the abdominal organs, a comprehensive examination of patients is carried out at the Yusupov Hospital:
- Ultrasound examination of the liver, pancreas, kidneys, adrenal glands;
- Multislice computed tomography of the abdominal organs;
- Chest X-ray;
- Bone scintigraphy.
In unclear cases, diagnostic laparoscopy is performed.
Small intestinal cancer is differentiated from benign tumors, intestinal tuberculosis, occlusion of mesenteric vessels, and Crohn's disease. In women, differential diagnosis is carried out with neoplasms of the uterus and appendages.
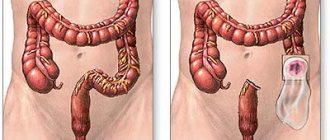
Treatment of small intestine cancer
The issue of choosing a treatment method for patients with malignant tumors of the small intestine is decided collectively at a meeting of the expert council with the participation of professors and doctors of the highest category. If small intestinal cancer is operable, surgeons perform a wide resection of the affected area of the intestine and lymph nodes, and excise the mesentery. The length of the small intestine allows radical removal of the tumor within the boundaries of healthy tissue. The integrity of the digestive tract is restored by performing enterocoloanastomosis (small intestine into large intestine) or enteroenteroanastomosis (small intestine into small intestine).
If duodenal cancer is detected, duodenectomy is performed, sometimes with distal gastrectomy or pancreatic resection. In case of advanced small intestinal cancer, where radical resection is not possible, a bypass anastomosis is performed between unaffected loops of intestine. The surgical stage of treatment of small intestine cancer is supplemented with chemotherapy. The same method in some cases is the only way to treat inoperable malignant tumors.
The long-term prognosis for small intestine cancer is determined by the stage of the cancer process and the histological structure of the tumor. In the presence of localized tumor processes without regional and distant metastases, the five-year survival rate after radical resection is 35-40%.
How to check the small intestine for a tumor? Call the Yusupov Hospital and doctors will conduct a comprehensive examination. Once the diagnosis is confirmed, multidisciplinary treatment will be selected for you. When small intestinal cancer is detected in the early stages during a screening examination, when there are no symptoms of the disease, oncologists have the opportunity to perform radical surgery. After it, the prognosis improves.
Stages
The stages of small intestinal cancer are presented using the example of adenocarcinoma. For GI stromal tumors or carcinoids, a different staging system may be used.
| Stage | Grouping by TNM | Description |
| 0 | Tis N0 M0 | Neoplasm only in the epithelium (the upper layer of mucosal cells). It has not grown into the deeper layers of tissue (Tis). No spread to regional lymph nodes (N0) or distant parts of the body (M0). |
| I | T1 or T2 N0 M0 | The neoplasm has grown into the deeper layers (lamina propria or submucosa) (T1), or through the submucosa into the muscularis propria (T2). No spread to regional lymph nodes (N0) or distant parts of the body (M0). |
| IIA | T3 N0 M0 | The neoplasm grew through the muscularis propria into the subserosal layer. No invasion into any adjacent organs or structures (T3). No spread to regional lymph nodes (N0) or distant parts of the body (M0). |
| IIB | T4 N0 M0 | The tumor has grown through the outer layer of tissue lining the intestine (serous or visceral peritoneum) or into adjacent organs or structures (T4). No spread to regional lymph nodes (N0) or distant parts of the body (M0). |
| IIIA | Any T N1 M0 | The neoplasm has grown into any layers of the intestinal wall (Any T). There is spread to 1 or 2 regional lymph nodes (N1) but not to distant parts of the body (M0). |
| IIIB | Any T N2 M0 | The neoplasm could grow into any layers of the intestinal wall (Any T). It has spread to 3 or more regional lymph nodes (N2) but not to distant parts of the body (M0). |
| IV | Any T Any N M1 | The neoplasm can grow into any layers of the intestinal wall (Any T). There may or may not be spread to adjacent lymph nodes (Any N). Spread to distant lymph nodes or organs such as the liver or peritoneum (inner lining of the abdomen) (M1). |