Hodgkin's lymphoma is a malignant disease of the lymphatic system. This name was first introduced by the World Health Organization not so long ago, in 2001. But this type of cancer was first described by a British physician and one of the founders of preventive medicine, Thomas Hodgkin.
in 1832. This disease is also called lymphogranulomatosis and malignant granuloma.
Hodgkin's lymphoma is characterized by enlarged lymph nodes, in which there is an uncontrolled accumulation of so-called tumor lymphocytes. During the development of the disease, there is a violation of the division and maturation of B-lymphocytes responsible for the production of antibodies. Atypical cells can also enter the circulatory system, which carries them to other organs. When they enter a new area of the body, they do not stop dividing and form a new tumor.
Since lymph nodes are located throughout the body, cancer can form in any of the internal organs and is localized in the chest, abdominal, axillary and groin areas. The most common lesions are the lungs, bones and liver.
five forms in total
:
- nodular sclerosis is the most common form. It has a relatively favorable course and in most cases responds well to treatment;
- lymphocytic predominance is less common, but also in many cases responds well to treatment;
- The mixed-cell form is less common and is most often diagnosed in people with HIV infection. This type of cancer is more aggressive and difficult to treat.
- Lymphocytic depletion is most common in older people and is often detected in the fourth and fifth stages of cancer;
- nodular with lymphoid predominance occurs much more often in men than in women. In more than 80% of patients, the disease is detected at stage I or II, which gives hope for a favorable outcome.
What is non-Hodgkin's lymphoma
Non-Hodgkin's lymphomas
is a large group of malignant neoplasms that develop from lymphocytes. To put it simply, these are cancerous tumors that affect the lymph nodes.
There are more than 30 varieties of this pathology. All of them have significant differences in clinical course. Among them there are both aggressive, rapidly progressing, and indolent, that is, growing very slowly.
In addition to the non-Hodgkin type of malignant lymphomas (NHL), the modern classification distinguishes Hodgkin's disease
(lymphogranulomatosis). How do these types of lymph node tumors differ from each other, and which one is more dangerous? Both of them begin in lymphoid tissues and can gradually spread to other organs. The difference between them lies in the fact that non-Hodgkin lymphomas much more often than Hodgkin lymphomas grow into extradontal organs (lungs, liver, spleen, etc.). That is, their main characteristic is that they are not located in one place. After the formation of NHL, it begins a journey through the blood and lymph throughout the human body.
Also, this type of neoplasm tends to have the highest degree of malignancy and, in the absence of adequate and timely therapeutic intervention, the pathology becomes fatal.
Risk of pathology
increases in the following cases:
— congenital and acquired diseases of the immune system;
— age over 60 years;
- obesity;
- exposure to chemical carcinogens (herbicides, benzene, etc.).
Causes and mechanism of development of non-Hodgkin lymphomas
The causes of most lymphomas remain unknown. There are a number of etiological factors common to all tumors that can contribute to the occurrence of NHL:
- Ionizing radiation.
- Chemicals with carcinogenic properties.
- Unfavorable environmental factors.
The viral nature of some forms of lymphomas has been proven, in particular, Burkitt's lymphoma (Epstein-Barr virus), some T-cell lymphomas (retrovirus HTLV-1).
Approximately 90% of cases of gastric MALT lymphoma (extronodal B-cell lymphoma) are associated with H. pylori infection.
The risk of developing lymphomas is increased in immunodeficiency conditions of various natures (HIV infection, autoimmune and hereditary diseases, etc.).
An immune cell, under the influence of causative factors, stops at some stage of maturation, transforms into a malignant one and begins to divide uncontrollably, which leads to the formation of a tumor. Non-Hodgkin's lymphomas begin with a single tumor focus, which is most often localized in a lymph node (nodal lesion), less often in other organs and tissues (extranodal lesion).
Over time, hematogenous (with blood flow) or lymphogenous (with lymph flow) spread of the tumor occurs, involving the bone marrow and central nervous system in the process.
Symptoms of non-Hodgkin's lymphoma
The appearance of this disease in the early stages can be suspected by the painful swelling of one or more lymph nodes. Most often they are found in the groin, armpits or neck.
The following symptoms may also occur:
:
- Unexplained weight loss;
- Loss of appetite;
- General weakness;
- Fever and night sweats.
Symptoms and signs
There are several typical signs of non-Hodgkin lymphoma.
Such symptoms, along with swelling of the lymph nodes and the appearance of pain in them, require immediate consultation with an experienced specialist. The greatest attention should be paid to the following symptoms and signs, which may indirectly indicate the development of NHL in a patient:
- Unexplained increase in body temperature above 38°C. This symptom is always accompanied by fever and night sweats. It is these signs that are protective and indicate that the immune system is trying to eliminate the emerging source of infection;
- A fairly common symptom indicating the development of non-Hodgkin lymphoma is facial swelling. It occurs due to compression of the ureter by enlarged lymph nodes located in the abdominal cavity. This leads to impaired urinary flow and secondary renal failure;
- Another typical sign that may indicate the development of NHL is anemia. It occurs due to internal bleeding accompanying the mutation of lymph cells located in the gastrointestinal tract.
Classification of non-Hodgkin's lymphomas
The diagnosis of non-Hodgkin lymphoma implies that the patient has one of the many subtypes of this pathology. They all differ in their histological picture (changes in the structure of mutated tissues and cells) and specific symptoms. In this regard, approaches to their treatment should be different.
Only a correctly performed diagnosis can most accurately determine what type of non-Hodgkin lymphoma a patient has.
The NHL is classified according to the following criteria
:
- The rate of disease development.
Here we distinguish between
indolent lymphomas
(which have a very slow course and may not manifest themselves for years) and
aggressive ones
(with accelerated development and spread. Their impact on the body is very dramatic).
There is also an intermediate form of NHL,
in which the pathological influence increases gradually; - The site of origin of the cancer
.
Their classification includes 2 types. Nodal
- those that developed directly in the lymph nodes and
extranodal
- outside them. The latter include non-Hodgkin lymphomas of the spleen, lungs, stomach, etc.
Most often, there are several classes of lymphomas, which I would like to talk about separately.
B cell lymphoma
This type of pathology appears as a result of mutation of B lymphocytes. Their main purpose in the human body is to maintain immunity. Thanks to them, a so-called “library of dangers” is formed in our bodies. When a patient is diagnosed with B-cell lymphoma, this indicates that the cells that recognize foreign bacteria and viruses have mutated. To put it simply, the development of non-Hodgkin B-cell lymphoma leads to the body losing the ability to fight even the simplest diseases.
Diffuse
This aggressive type of NHL is the most common. It can occur at any age and has various symptoms. The tumor received this name because it causes a complete disruption of the internal structure of the lymph node. This leads to the rapid spread of mutated cells to all parts of the lymphatic system, that is, their peculiar “diffusion” occurs. In diffuse non-Hodgkin lymphomas, malignant neoplasms appear either at all points where the nodes are concentrated, or in any single area. The tumor that appears there grows rapidly and in a short time leads to the appearance of painful symptoms.
Large cell
Large cell non-Hodgkin lymphoma most often appears as a painless but rapidly growing tumor in the groin area, armpits, or neck. As it grows, it begins to be accompanied by symptoms such as significant weight loss, fever and night sweats. This type of tumor grows very quickly.
Follicular
The name of this type of non-Hodgkin lymphoma comes from the place of its formation - the follicles of the epidermis (hair follicles). For the most part, the disease is characterized by nodal localization, that is, it does not extend beyond the lymph nodes and does not grow into other organs. Its flow character is indolent. The development of follicular non-Hodgkin lymphoma is very slow and secretive. This is the biggest danger of this type of cancer. For the most part, it can be identified only in the final stages, when metastasis has occurred into various internal organs.
Small cell
This type of pathology develops when small cells of the lymphatic system mutate. Small cell lymphoma is characterized by a slow progression of malignancy. It has practically no specific symptoms and is most often detected in the last stages. For this reason, its complete cure can be difficult.
Brain lymphoma
This type of non-Hodgkin's lymphoma occurs mostly as a secondary lesion. It occurs as a large tumor formation in the head and is characterized by the following accompanying symptoms:
— Impaired sensitivity and coordination of movements;
- Severe headaches;
- Loss of memory and cognitive abilities.
A characteristic feature of brain lymphoma is the difficulty of diagnosing it due to the complexity of performing a biopsy. It is not always possible to quickly obtain the tumor material necessary for research.
Lymphoma of the lung
The symptoms of this type of disease in the first stages resemble a cold, accompanied by fever, cough with slight sputum, general weakness and sweating. The development of lung lymphoma can be suspected only by the worsening condition of the lymph nodes. They noticeably increase in size and become painful upon palpation. In the last stages of pulmonary lymphoma, patients experience hemoptysis. Metastasis also occurs to neighboring organs and the spinal cord. In the case when the pathology is diagnosed at the initial stage of the formation of the tumor process, almost all patients have a good chance of a complete recovery.
Stomach
Quite a rare type of pathology. It is characterized by the tumor growth of lymph cells occurring in the stomach. Damage to the digestive organ can be not only primary, but also secondary. Gastric lymphoma is characterized by the appearance of symptoms typical of diseases of the gastrointestinal tract: decreased appetite, nausea, turning into vomiting and abdominal pain. This makes it possible to identify this type of non-Hodgkin lymphoma in the early stages and, accordingly, carry out the most successful treatment.
Mediastinum
A very rare type. A feature that characterizes primary mediastinal lymphomas is the tendency to rapid growth and spread to the affected organ, located in this area, the esophagus, trachea, large bronchi, heart, etc. In this case, they are compressed, causing shortness of breath, cough, chest pain and dysphagia ( swallowing disorders). Non-Hodgkin's lymphoma of the mediastinum occurs mostly in young women. They suffer from this type of pathology 2 times more often than men.
T cell
This type of tumor is characterized by a mutation of T lymphocytes, which are responsible for destroying foreign pathogenic cells in the body. It manifests itself in generalized (general) enlargement of lymph nodes and skin lesions. Skin eczema appears as papules and plaques. At the same time, anemia and bone marrow damage are not typical for this form of pathology.
Chronic non-Hodgkin's lymphoma
A chronic course is characteristic of indolent (sluggish) lymphomas. The course of the pathology in this case is unpredictable. The remission stage is not stable. An exacerbation can begin at any moment. The chronic form of lymphoma is characterized by a low content of tumor cells in the blood and moderate lymphocytosis. Life expectancy in the absence of adequate treatment reaches several years until the disease becomes acute.
MALT lymphomas (tumors of mucosal associated lymphoid tissue) are B-cell non-Hodgkin's lymphomas (NHLs) of marginal zone origin, along with marginal zone lymphomas of the spleen and nodal marginal zone lymphomas. Moreover, MALT lymphomas are the most common type of marginal zone lymphomas, accounting for 50–70% of all cases [1, 2].
It should be noted that lesions of the gastrointestinal tract in NHL are observed, according to the literature, in 4-25% of cases of all extranodal localizations of the pathological process. At the same time, the number of NHL among all malignant neoplasms of the gastrointestinal tract (GIT) ranges from 1 to 10%. MALT lymphomas account for 6–11% of NHL in the gastrointestinal localization [2–4].
The most common form of MALT lymphoma of the gastrointestinal tract is gastric MALT lymphoma, which accounts for 30-40% of all cases of this disease. Intestinal lesions are found in 4-8% of patients with MALT lymphomas, and the disease occurs in the small intestine 2 times more often than in the large intestine. Among extraintestinal localizations of MALT lymphomas, lesions of the head and neck, skin, lungs, thyroid and mammary glands are of leading importance [5–7].
The main role in the pathogenesis of MALT lymphomas, according to modern concepts, is assigned to a chronic inflammatory process, leading to the accumulation of autoreactive lymphoid tissue, repeated division of B cells with an increase in the number of cytogenetic disorders, which leads to the development of malignancy [2, 6]. The main causes of the chronic inflammatory process as an inducer of the development of MALT lymphomas are considered to be autoimmune processes and the presence of persistent infection. For lymphomas localized in the gastrointestinal tract, a connection between Helicobacter pylori
and the risk of developing gastric MALT lymphomas (
H. pylori
in gastric MALT lymphoma is detected in 90% of patients).
In addition, a correlation has been identified between the presence of Helicobacter jejuni
and the development of duodenal lymphomas [5, 6, 8]. There are reports indicating an increased likelihood of the disease in patients with chronic viral hepatitis C [8]; provides data on the possibility of the appearance of intestinal lymphomas against the background of celiac disease [9].
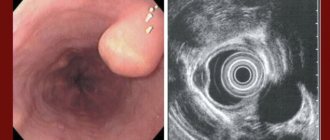
From the point of view of the clinical picture of the disease, MALT lymphomas of the gastrointestinal tract are characterized by a long asymptomatic course and can also be accompanied by a number of nonspecific symptoms. When the stomach is affected, the disease can occur under the guise of gastritis; when localized in the intestines, the main complaints of patients may be a feeling of discomfort in the abdomen, moderate periodic pain, and dyspepsia. In some cases, signs of malabsorption appear [2, 6, 10, 11].
Among the complications of intestinal MALT lymphomas, the leading role is played by intestinal obstruction, which, according to some data, develops in 70-80% of patients. Other acute life-threatening conditions such as tumor perforation and bleeding are relatively rare (1-3% of cases) [2, 4, 7].
The principles of treatment of MALT lymphomas of the gastrointestinal tract depend on the location of the formation and the stage of the malignant process. When the stomach is affected, the main treatment method is anti-Helicobacter therapy, which in 50-80% of cases allows one to achieve remission. In case of ineffectiveness of eradication therapy, as well as in case of a high degree of malignancy of the tumor, combined treatment (chemotherapy, radiation therapy, surgery) is recommended [3, 5, 6]. When lymphoma is localized in the intestine, surgical techniques, radiation, mono- and polychemotherapy, and combined treatment are used. The role of surgical treatment of lymphomas of the small and large intestine is especially high due to a significant proportion of complications requiring urgent surgical intervention [1, 2, 8].
We have experience in treating a patient with MALT lymphoma of the small intestine, which was first identified due to tumor perforation and the development of the clinical picture of peritonitis. Here is our observation.
Patient P., 70 years old, was hospitalized on April 16, 2012 in the surgical department of the Central Clinical Hospital of the Federal Customs Service of Russia (CCG FCS) with complaints of severe abdominal pain, worsening with changes in body position, cough, nausea, and general weakness.
From the anamnesis it is known that from August 26, 2010 to September 9, 2010, the patient was hospitalized in the therapeutic department of the Central Clinical Hospital of the Federal Customs Service for fever and anemia of unknown origin. The fever first appeared in August 2010 and was characterized by evening rises in body temperature to 39.0–39.5 °C and night sweats. The hemoglobin level in the blood during hospitalization was 98 g/l. Since 1980, the patient was diagnosed with chronic viral hepatitis C, and since 1989 - celiac disease. After a course of anti-anemic therapy, the patient was voluntarily discharged for outpatient treatment. However, due to ongoing fever, on September 20, 2010, the patient was hospitalized at an outside medical facility, where during the examination, hematological, oncological and rheumatological causes of the disease were rejected. Enteritis not specified in the context of celiac disease or an abscess of unknown localization were identified as a possible factor causing the fever. The patient refused further examination at this healthcare institution and on November 11, 2010 she was again admitted to the therapeutic department of the Central Clinical Hospital of the Federal Customs Service with continuing nightly fever. At the same time, the patient noted that over the previous 3 months she had lost 10 kg. In the results of laboratory tests, attention was paid to leukocytosis (up to 12 thousand) with a band shift (up to 22%), hypoproteinemia (50 g/l), and a positive reaction to occult blood in a stool test. During the hospital stay, esophagogastroduodenoscopy (superficial atrophic gastritis, signs of atrophic duodenopathy), colonoscopy (single diverticulum of the colon), computed tomography of the abdominal cavity and pelvis (signs of enteritis, quantitative enlargement of the lymph nodes (LN) of the mesentery of the small intestine, hepatomegaly, fatty hepatosis), enterography (no filling defects were detected). The patient was also repeatedly examined by specialist consultants from external therapeutic departments. Among the therapeutic measures, the patient underwent massive antibiotic therapy with a change in antibacterial drugs (ceftriaxone, amikacin, tienam). After prescribing each of the drugs, positive dynamics were observed in the form of normalization of body temperature and a decrease in leukocytosis, however, after discontinuation of the antibiotic, the symptoms returned. Due to this picture of the disease, therapy with prednisolone ex juvantibus
, during which regression of fever was obtained. The patient was discharged on December 30, 2010 for outpatient observation with recommendations to continue taking prednisolone. Diagnosis: celiac disease with maldigestion syndrome of the third degree, secondary iron deficiency anemia of moderate severity, chronic viral hepatitis C, class A, multinodular euthyroid goiter of the second degree, kidney cysts, ciscirculatory encephalopathy of the second degree, atherosclerosis of the brachycephalic arteries, autonomic dystonia syndrome.
From January 12, 2011 to January 19, 2011, a control examination was carried out in the therapeutic department of the Central Clinical Hospital of the Federal Customs Service. Among the patient's complaints, moderate general weakness remained; her body temperature remained normal while taking steroid hormones. A weight gain of 2 kg was noted. Upon discharge, it was recommended to continue taking prednisolone.
During this hospitalization in the surgical department of the hospital, upon examination of the patient, pronounced pain on palpation was determined in all parts of the abdomen, which was moderately swollen. Positive symptoms of peritoneal irritation were detected in all sections. Blood tests revealed leukocytosis (16.7 thousand), hypoproteinemia (44 g/l). Based on the results of a chest x-ray and a plain x-ray of the abdominal cavity, right-sided lower lobe pneumonia was diagnosed. No data were obtained to confirm horizontal fluid levels, intestinal arches, or free gas in the abdominal cavity.
Considering the clinical picture of diffuse peritonitis, the patient was operated on urgently after short-term preparation in the intensive care unit. Surgical intervention began with diagnostic laparoscopy. When examining the abdominal cavity in all parts, there is up to 500 ml of purulent turbid effusion, fibrin overlay. The loops of the small and large intestines are hyperemic, edematous, sluggishly peristalt, and moderately distended. Taking into account the prevalence and severity of the process, it was decided to perform an access conversion. A midmedian laparotomy was performed. No pathology was detected in the liver, gallbladder, pancreas, stomach, or colon. When examining the small intestine at a distance of 1.5 m from the ileocecal angle, a circular thickening of the intestinal wall of up to 4-5 mm over a distance of 6 cm was discovered without obstruction of patency. In the center of the formation, a perforated hole of up to 2 mm was identified, from which intestinal contents came. In the mesentery of the small intestine, in the projection of the tumor, a package of lymph nodes was identified, enlarged to 2-4 cm, with a soft elastic consistency. Intraoperative diagnosis: perforation of a tumor of the small intestine. Diffuse fibrinous-purulent peritonitis. The following was performed: resection of a section of the small intestine with a tumor with a 20 cm indentation to the sides of the tumor; wedge-shaped resection of the mesentery of the small intestine with lymph nodes. The intestinal stumps are sutured using a hardware suture, a side-to-side anastomosis is performed, the window in the mesentery is sutured with interrupted sutures. A nasointestinal tube was inserted 30 cm into the small intestine. The abdominal cavity was sanitized and drained, and the laparotomy wound was sutured tightly in layers.
The course of the postoperative period was complicated by the presence of community-acquired lower lobe pneumonia in the patient. Detoxification, massive antibacterial therapy, and physiotherapy were carried out. With treatment, the pneumonia resolved. The sutures were removed on the 11th day after surgery, the wound healed by primary intention. A control ultrasound of the abdominal organs revealed no free fluid, streaks, or infiltrates. Body temperature at discharge was within normal limits. Histological examination of the surgical material: large cell lymphoma (MALT lymphoma) of the small intestine with ulceration and perforation of the intestinal wall. No signs of tumor growth were found at the resection margins or mesenteric lymph nodes. In the lymph nodes, nonspecific reactive hyperplasia of the B-cell type is determined. The patient was discharged on May 4, 2012 in satisfactory condition under the supervision of an oncologist at her place of residence.
Thus, the presented case from practice demonstrates not the most typical course of such a rare disease as MALT lymphoma of the small intestine. The patient had very pronounced symptoms for a long time, the nature of which, however, did not allow us to assume and determine lymphoma of the small intestine. And despite the fact that the localization of the pathological process was determined correctly during previous examinations, the nature of the disease was not clarified before the occurrence of a surgical complication. This is primarily due to the low accessibility of the small intestine for standard endoscopic and imaging methods, while techniques such as intestinoscopy and capsule endoscopy remain rare. It is also interesting that the patient has a long history of celiac disease and chronic viral hepatitis C, which are reported to increase the risk of developing intestinal lymphomas.
As a result, it should be noted that various diseases of the small intestine, including MALT lymphoma, necessitate wider implementation of modern endoscopic technologies, which can prevent the development of life-threatening conditions during a long course of the pathological process and facilitate surgical treatment as planned, if any indications for performing the operation.
Stages of non-Hodgkin's lymphoma
To understand the extent of the disease, it is necessary to determine the stage of non-Hodgkin lymphoma. In the international classification of this disease, there are 4 of them: I and II are local, limited, and III and IV are widespread.
· I. Only one area may be involved in the lymphoma process. Only one lymph node increases in size and becomes inflamed. General symptoms, pain and weakness are absent;
· II–I. Tumors increase in size and become multiple. Also at this stage of non-Hodgkin lymphoma, general symptoms begin to appear;
· III. This stage of the development of the disease is characterized by the spread of malignant neoplasms to the chest and abdominal cavity. At this time, almost all internal organs are damaged;
· IV. The most severe stage of cancer. Mutated cells grow in the central nervous system and bone marrow. The prognosis in this case is not encouraging.
The letters “A” or “B” are always added to the stage number. This designation specifies the stage corresponding to the pathology. It also completes her picture. “A” the patient completely lacks any external signs of illness. “B”, specific symptoms appear, such as profuse night sweats, a significant increase in temperature, or unexplained weight loss.
Survival prognosis for stage 4
If you do not pay attention to the above symptoms in time and do not consult a doctor, the disease can develop to a severe fourth stage. Stage 4 is characterized by the spread of metastases in the bones, bone marrow, spinal cord, brain and other organs. However, even in this case, the probability that a person will live at least another 5 years is 65%, that is, in any case, you should not give up, but start treatment immediately. And it is better to do this with trusted doctors, for example, at ON CLINIC.
Thanks to advanced technologies and the latest equipment, MMC ON CLINIC specialists achieve excellent results and complete cure for the majority of patients.
Diagnosis of non-Hodgkin's lymphoma in Israel
In cancer centers of this country, the following diagnostic procedures are performed to identify the stage of NHL:
- Biopsy.
Taking a piece of tissue from the affected lymph node or organ. Thanks to it, it is possible to most accurately identify what type of pathology is present, non-Hodgkin's or Hodgkin's disease. This allows you to select the most adequate treatment; - In case of pathological accumulation of a large volume of fluid in the abdominal cavity or sternum, aspiration is performed.
This technique allows you to conduct a laboratory study of it and identify the cause of its appearance; - If there is a suspicion of central nervous system cancer, a lumbar puncture
. This is a sample of cerebrospinal fluid; - The PET-CT
method allows you to informatively determine the stage of spread of non-Hodgkin lymphoma throughout the body. Thanks to it, those areas where the metabolic process (metabolism) occurs abnormally quickly are quickly identified. This is direct evidence of the presence of mutated cells there; - Lymphangiography
. Examination of the lymphatic system using a contrast agent. This makes it possible to see the affected lymph nodes on radiographs. To detect the presence of NHL in the spinal cord and brain, Israeli specialists use the MRI (magnetic resonance imaging) method.
All diagnostic measures take from 3 to 5 days
. In each specific case, their duration is individual and depends on the stage of development of the disease.
Treatment of non-Hodgkin's lymphoma in Israel
All therapeutic measures that make it possible to prolong the life of a patient with this pathology are compiled in Israeli clinics on an individual basis. An integrated approach is implemented for each patient. Many people are interested in what the treatment protocols are. That is why this issue should be examined in more detail.
Treatment protocol for non-Hodgkin's lymphoma
In case of NHL, which almost always manifests itself very aggressively, Israeli oncology centers use 3 ways to solve the problem:
- Bone marrow transplantation;
- Lumbar punctures (taking cerebrospinal fluid) and injecting antitumor antibodies in their place;
- A combination of chemotherapy and radiotherapy.
Several specialists take part in the development of the therapy protocol, starting with an oncologist and hematologist, and ending with a psychologist and physiotherapist. In Israel, it is possible to use the following protocols in the treatment of non-Hodgin lymphoma, which are prescribed by a specialist based on the results of the examination:
- Routine;
- With the use of biological chemotherapy drugs.
Medicines can be administered both on an outpatient basis and during hospitalization. Usually 6 courses of therapy are prescribed. After the third one, a PET scan is performed.
Chemotherapy for non-Hodgkin's lymphoma
During this procedure, several medications are used. Their use is carried out simultaneously, which makes it possible to destroy a larger number of cancer cells. The combination is necessary due to the fact that different drugs have different effects on malignant neoplasms. A big advantage of chemotherapy carried out in Israeli cancer centers is the use of drugs that have virtually no side effects.
Targeted therapy for non-Hodgkin's lymphoma
Thanks to it, lymphoma cells begin to destroy, and the rate of their development slows down. During targeted therapy for the treatment of non-Hodgkin's lymphoma, Israeli specialists use highly effective monoclonal antibodies. These are Mabthera, Zevalin, Alemtuzumab. Interferon is also used in the treatment of NHL in these clinics.
Lymphomas: treatment
The development of lymphoma treatment tactics by CELT specialists is based on the diagnostic results obtained and the patient’s individual indications. It may include surgery, radiation and chemical therapy:
| Treatment method | What is? |
| Radiation therapy | Indicated independently exclusively for localized forms of pathology and low degree of malignancy of the neoplasm. It can be used in cases where other methods of treatment are not available for one reason or another. |
| Chemotherapy | Most often it begins with the use of several cytostatic drugs of different groups. It can be carried out independently or in combination with radiation therapy, which allows achieving longer remissions. As a rule, it requires two to three courses in order to achieve complete remission. |
| Operations | Indicated for isolated lesions of internal organs, most often the gastrointestinal tract. They are aimed at complete or partial removal and require chemotherapy. |
| Additional |
|
At CELT, consultations are conducted by hematologists of the highest category, candidates and professors of medical sciences with many years of experience in practical and scientific work. You can schedule a consultation with them online or by phone. No less qualified specialists work in the urology department of our clinic. You can contact them and solve any delicate problem that reduces the quality of your life. They can undergo a diagnostic procedure such as cystoscopy of the bladder.
At CELT you can consult a hematologist.
- Initial consultation – 3,200
- Repeated consultation – 2,000
Make an appointment
By making an appointment with a hematologist, you can get a comprehensive consultation. The doctor is competent to treat various blood diseases, most of which can be identified in the early stages and prescribe timely treatment to cope with the disease quickly and easily.
Non-Hodgkin lymphoma prognosis
The prognosis for this pathology directly depends on the stage of the disease and the treatment provided. Recently, there has been an increase in patients with five- and ten-year survival rates.
Relapse of non-Hodgkin's lymphoma
Exacerbation of the disease indicates a significant deterioration in the prognosis. When non-Hodgkin's lymphoma relapses, especially in young patients, emergency brain transplantation is used. This significantly increases the chances of further continuation of life.
Non-Hodgkin's lymphoma, how long do they live?
This question worries many patients. The life expectancy of a person with NHL depends on the type of pathology, the location of its source, the timeliness of treatment and the correctness of the selected treatment protocol. According to the latest statistics, 80 out of 100 patients with non-Hodgkin lymphoma survive more than a year, 65% more than 5 years and 54% more than 10 years after diagnosis.
Is it possible to give birth after non-Hodgkin's lymphoma?
Pregnancy does not affect the course of NHL, just as they do not affect it at all. If the pathology does not progress, all therapeutic measures can be postponed for the period of bearing the child. Symptomatic therapy is also used during pregnancy in patients with non-Hodgkin's lymphoma. With its help, it is possible to significantly improve the mother’s condition, on which the prognosis for the child largely depends.
Non-Hodgkin's lymphoma. Recommendations after treatment
This issue also worries patients. Many people who have undergone therapy after being diagnosed with non-Hodgkin lymphoma fall into a state of depression or anger at the world around them. Neither one nor the other is worth doing. Many patients with this diagnosis, after undergoing courses of therapy, live for many years with virtually no disruption to their quality of life. The only thing required is to follow the recommendations of the specialists who performed the treatment.