Rectal cancer is a malignant neoplasm that occurs 15-20 cm from the anus. It ranks second in mortality among the most common types of cancer pathologies. The danger of the disease lies in late diagnosis, since in the initial stages it actually does not manifest itself, like colorectal cancer. Stages zero and one of oncology are best treated.
While lung cancer is more common in men, breast cancer is more common in women, and colorectal cancer is equally common in both sexes. According to statistics, in the Russian Federation there are about 75 cases of this disease per 100,000 inhabitants.
The tumor has a normal mechanism of development, characteristic of many oncological diseases.
Malignant cells affect the mucous epithelium of the intestine, since it is here that stagnation of feces and inflammatory processes that appear as a result of injury to the intestinal lining can be observed. IMPORTANT:
The risk of developing colorectal cancer increases with age. Particular caution is required for people over 50 years of age. They are recommended to undergo an annual medical examination, which will include a mandatory colonoscopy and a visit to a proctologist.
Determination of tumor markers
One of the modern methods for diagnosing colorectal cancer is research using tumor markers. The study of tumor markers specific to rectal cancer is used in making a diagnosis, assessing prognosis and the effectiveness of treatment.
Analysis of the level of serum CEA (cancer embryonic antigen) before surgery makes it possible to predict the further course of the disease in patients with stages II-III.
Determination of TIMP-1 and suPAR markers is used in the diagnosis of rectal cancer for prognosis and deciding on the prescription of postoperative adjuvant chemotherapy for patients with the initial stages of the disease. The results of the studies showed that in patients with disease stage no higher than II/B (according to Dukes) and low levels of TIMP-1 and suPAR, the lifespan after surgery is comparable to the lifespan of a healthy person of the same age. Such patients, as a rule, do not require any additional treatment.
Causes of the disease
One of the main causes of this cancer is polyps (glandular growths). They develop on the wall of the rectum and, over time, can degenerate into a malignant tumor.
Main causes of rectal cancer:
- Hereditary factor (presence of genetic syndromes - familial adenomatous polyposis, Crohn's disease).
- The presence of other neoplasms in the body.
- Diabetes.
- Papilloma virus.
- Immune system deficiency.
- Abuse of alcoholic beverages, smoking.
- Inflammatory diseases in the intestinal area.
- Work in hazardous industries with chemicals.
- Sedentary lifestyle.
- Diseases of the gastrointestinal tract.
The risk group includes people with benign intestinal tumors. They need to undergo preventive treatment, which will not allow the tumor to degenerate. A sedentary lifestyle also negatively affects the condition of the body, increasing the possibility of developing a pathological condition.
Sigmoidoscopy, sigmoidoscopy and colonoscopy
Endoscopic examinations are the main methods for diagnosing rectal cancer at an early stage. During the procedure, the doctor gets the opportunity to:
- examine the intestinal walls;
- remove a small polyp (up to 1 mm) and send it for biopsy;
- take small fragments of tissue from other suspicious areas of the mucous membrane for analysis.
Diagnosis of rectal cancer can be done using a rigid sigmoidoscope, sigmoidoscope (flexible sigmoidoscope), or colonoscope.
If the required equipment is available, the initial examination is usually performed using a sigmoidoscope: a flexible device expands the doctor's capabilities and reduces the patient's discomfort during the procedure. However, such a device, like a rigid sigmoidoscope, is limited in length. In this regard, a specialist can examine only the lower parts of the large intestine - the rectum and sigmoid colon.
Therefore, if an extensive examination is necessary, including examination of the overlying parts of the intestine, a longer device is used - a colonoscope.
Each of the listed methods (sigmoidoscopy, sigmoidoscopy and colonoscopy) for diagnosing rectal cancer can be detected at the asymptomatic stage of the disease and can be included in preventive examination schemes.
Symptoms of colorectal cancer
Finding signs of cancer at an early stage can significantly improve your prognosis. You should carefully monitor your health and if you notice any suspicious symptoms, consult a doctor immediately.
Main symptoms of rectal cancer:
- change in bowel regularity;
- diarrhea or constipation;
- blood or mucus in stool;
- pencil chair;
- digestive problems (flatulence, abdominal cramps);
- fatigue;
- frequent or painful gas;
- pain during bowel movements;
- frequent urge to go to the toilet;
- feeling of poor bowel movements.
IMPORTANT:
the above symptoms do not necessarily mean the presence of cancer. They can also be caused by a polyp, inflammation of the intestine, hemorrhoids. However, if any of these signs appear, consult a physician or gastroenterologist.
At an early stage, symptoms are intermittent. As the symptoms progress, they become more severe, including:
- anemia occurs;
- a person loses weight for no reason;
- there is chronic poor health.
The specificity of symptoms and the intensity of their manifestation depend on the location of the tumor, the stage of the disease and the degree of damage to other organs. Oncology manifests itself most clearly in an advanced state.
CT colonography
This method is also called virtual colonoscopy. The study is carried out using a computed tomograph. Before scanning, air is pumped into the appropriate area of the intestine to straighten the folds. After this, a series of images are taken, on the basis of which a 3-dimensional image of certain areas of the intestine is constructed. CT colonography is more comfortable and safe for the patient, but cannot always replace endoscopic examination, since it does not make it possible to perform a biopsy.
About the disease
The mucous membrane of the final portion of the colon is covered with columnar epithelium with a large number of glands. Their cells produce mucus. Under the influence of risk factors, pathological cells appear with uncontrolled division and loss of the apoptosis mechanism - programmed death. Gradually, a tumor of the rectum is formed from them.
Presumably the causes of rectal cancer have been established:
- Poor nutrition. The predominance of meat foods and animal fats in the diet with a simultaneous deficiency of plant fiber impairs the passage of feces, contributes to constipation and the development of colorectal tumors.
- The role of heredity has been noticed in the occurrence of certain forms of neoplasms.
- Precancerous pathologies - polyps, Crohn's disease, ulcerative colitis.
- Immunodeficiency conditions, carcinoma of the genital organs or breast in women.
Biopsy
Diagnosis by biopsy for rectal cancer allows us to determine the presence, type and degree of malignancy of tumor cells. According to the latest indicator, neoplasms are usually divided into 3 categories:
- 1 – slow-growing cancerous tumors with a low degree of malignancy and a low likelihood of spreading outside the intestine;
- 2 – moderately fast growing tumors with an average probability of spreading beyond the intestine;
- 3 – fast-growing neoplasms with a high probability of spreading outside the intestine.
If a biopsy reveals low-grade atypical cells (grade 3 malignancy), there is a high probability of not only the spread of cancer to other tissues and organs, but also recurrence of the disease after surgery. Such patients are usually prescribed complex treatment regardless of the stage of the disease.
How to treat colorectal cancer
The most common method used to treat colon cancer is surgery. Surgical treatment is supplemented with radiation or chemotherapy.
Surgical care for rectal cancer is divided into 3 types:
- For small tumors, endoscopic excision is possible. This tactic is used only in the presence of a neoplasm that has affected the mucous and submucosal layers.
- A popular, new method is transanal endomicrosurgery. Doctors are trying to preserve the intestinal walls. The recovery period after surgery is easily tolerated by patients.
- A section of the intestine is completely excised if the malignant tumor has affected the muscle layer. In addition to the tumor itself, surrounding lymph nodes and some healthy tissue are removed.
IMPORTANT:
In most cases of rectal cancer, the tumor does not allow the natural anus to be preserved. In this case, the doctor forms a colostomy - the intestines are removed to the anterior abdominal wall. Over time, some patients may undergo repeat surgery to reconstruct their intestines.
Surgical treatment is almost never supplemented with radiation therapy. But this technique is actively used in the treatment of rectal cancer. The reason for this is the low mobility of this part of the intestine, which makes it possible to direct the rays directly to the location of the tumor.
Ultrasound and CT
Ultrasound for rectal cancer is prescribed to clarify the diagnosis and extent of the process. The examination can be carried out in the usual way (through the anterior wall of the abdomen), as well as with a rectal sensor. An ultrasound examination of the rectum is most informative when assessing the condition of nearby lymph nodes.
If there is a suspicion that the process has spread to other organs, a computed tomography (CT) scan of the abdomen and chest is performed to determine metastases in the liver and lungs.
If you need a second opinion to clarify your diagnosis or treatment plan, send us an application and documents for consultation, or schedule an in-person consultation by phone.
+7 499 490-24-13
Expert opinion
Diagnostic methods
Patients suspected of having rectal cancer should immediately undergo a comprehensive examination and receive recommendations from an oncologist.
Diagnostics includes:
- Examination of the patient and collection of complaints. As a rule, the patient first visits a therapist, and only then goes to an appointment with a specialized specialist - a proctologist, oncologist-surgeon. The doctor will examine the nature of the symptoms and prescribe the necessary tests.
- Tests are prescribed: a general blood and urine test, a biochemical blood test and tumor markers for colorectal cancer. Studies make it possible to assess the general condition of the internal systems of the body, detect foci of inflammation and the extent of their prevalence.
- Investigations: colonoscopy or irrigoscopy, magnetic resonance or computed tomography, and ultrasound examination of the abdominal cavity. Allows you to determine the size of the tumor and its location.
- Screening methods. This type of research allows you to identify pathology before the first symptoms appear. This is a digital examination, endoscopy, stool analysis for occult blood.
After tests and studies are completed, observation and treatment is carried out by an oncologist.
IMPORTANT:
Additionally, the oncologist can send the patient for a biopsy. The procedure involves taking a piece of tumor tissue, which is sent for laboratory testing.
Classification
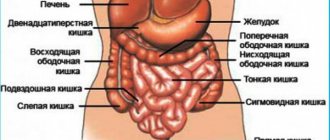
The rectum is the final segment of the large intestine, which starts from the sigmoid colon and ends at the anus. Stool accumulates in the rectum. In men, this section of the intestine is adjacent to the prostate gland, seminal vesicles and bladder, and in women – to the posterior wall of the vagina and uterus.
Based on the type of growth, the following forms of malignant tumors are distinguished:
- Endophytic - grows in the thickness of the wall of the rectum;
- Exophytic – grows into the intestinal lumen, eventually causing obstruction;
- Saucer-shaped - combines both types of tumor growth, occurs in the form of a tumor-ulcer.
The following histological types of rectal cancer are distinguished:
- Adenocarcinoma;
- Mucous adenocarcinoma;
- Glandular squamous cell carcinoma;
- Basal cell carcinoma;
- Mucocellular cancer;
- Squamous cell carcinoma;
- Undifferentiated cancer;
- Unclassified cancer.
The most common is adenocarcinoma of the rectum. Poorly differentiated squamous cell carcinoma consists of mutated squamous epithelial cells; they can be keratinized or non-keratinized. The appearance of the tumor resembles an ulcerative formation, in some cases cauliflower. Ulceration of the tumor indicates a high malignancy of the rectal tumor.
Squamous cell carcinoma has symptoms similar to those of hemorrhoids and anal fissures. A poorly differentiated form of squamous cell carcinoma is a highly malignant cancer that tends to rapidly metastasize, affecting nearby organs and tissues, as well as distant ones. The poorly differentiated form of squamous cell carcinoma is prone to relapses, which very often occur in the first two years after treatment.
Treatment before and after surgery
Chemotherapy and radiation therapy are indicated for patients with stage 2 or higher tumors.
If before the operation metastases were detected in several lymph nodes, and the tumor has grown into the muscle layer, then at the stage of preparation for the operation a short course of radiation therapy is carried out for 5 days. This allows you to destroy early metastases and reduce the size of the formation itself.
Treatment of rectal cancer after surgery is carried out after obtaining pathomorphological data on the removed tissues. The issue of radiation or its combination with chemotherapy is being decided. Radiation therapy after surgery destroys the remaining cells in the area of the primary tumor and prevents its recurrence. In inoperable patients, it alleviates the condition.
Sensitivity to chemotherapy is detected in 30% of patients. It is prescribed for therapeutic purposes to destroy metastases.
Chemotherapy is also carried out adjuvantly - to prevent the spread of carcinoma if damage to several lymph nodes is detected. This method of therapy improves the quality and life expectancy of patients with metastases. Platinum preparations, 5-fluorouracil, leucovarin, and calcium folinate are used. Medicines are administered intravenously in courses of several days. Chemotherapy is also used in combination with radiation before surgery for locally advanced cancer. This combined treatment is carried out for 1-1.5 months, and after the end of irradiation, surgery is performed 6 months later.
Symptoms
Signs of rectal cancer, the first symptoms do not appear immediately. The initial stage of tumor development is characterized by a certain discomfort and symptoms similar to those of various intestinal diseases. Often the first symptoms of a tumor are:
- The appearance of streaks of blood in the stool, which appear due to damage to the neoplasm by feces;
- Pain;
- Diarrhea or constipation.
The initial symptoms of colorectal cancer are often ignored. Several years pass from the onset of tumor development to the appearance of pronounced symptoms. The tumor slowly invades the organ, then grows into its wall and affects surrounding tissues and organs - about two years pass from the beginning of growth to its metastasis.
As the tumor grows, symptoms become more severe. Patients develop persistent constipation or diarrhea, and the shape of stool changes. Then the temperature rises, the skin turns pale, and jaundice develops. Nausea, vomiting, and pain during bowel movements occur. The patient loses his appetite and his weight decreases. Over time, chronic or acute intestinal obstruction develops.
Cancer can affect the rectosigmoid, ampullary and anal parts of the rectum. The clinical picture of the disease will be different in each case. In the supramullary region, scirrhous forms of cancer are more often observed. They often cause a narrowing of the intestinal lumen. Small neoplasms are manifested by the following symptoms:
- Constipation;
- Feeling of incomplete bowel movement;
- Urge to defecate.
Constipation may be followed by diarrhea with blood or mucus. As the narrowing progresses, the phenomena of partial, less often complete, intestinal obstruction develop. In some cases, intestinal obstruction is the first symptom of rectal cancer in men or women.
If the cancerous tumor is located in the ampulla of the rectum, the disease proceeds secretly. With ampullary localization of cancer, the dominant symptom is the release of blood and mucus during bowel movements. Blood usually appears with the first portions of stool or before bowel movements. Its type and quantity are variable. Most often these are streaks of blood or spotting.
Causes of pain
Pain in bowel cancer is observed in 80% of patients. In some cases, symptoms are similar to the following diseases:
- Acute appendicitis;
- Peptic ulcer of the stomach or duodenum;
- Colic in urolithiasis, cholelithiasis.
The pain may be combined with muscle tension in the anterior abdominal wall, fever, vomiting and nausea. An increase in pain occurs with an increase in tumor size, tumor growth into neighboring organs and tissues, with the development of intestinal obstruction, the development of an inflammatory process in the tumor, or an abscess.
Symptoms of advanced colorectal cancer
When a tumor ulcerates and disintegrates under the influence of infectious agents, the tumor often becomes inflamed and suppurates. This is accompanied by the appearance of constant pain in the lower back, rectum, and deep pelvis. The pain intensifies during bowel movements. Discharge from the anus becomes bloody-purulent and foul-smelling. A feeling of delayed bowel movements and painful tenesmus are often associated.
If a large tumor narrows the lumen of the rectum, feces are released in the form of a narrow column resembling a pencil. When the anorectal region, rich in nerve endings, is affected by a malignant neoplasm, pain in the anus during bowel movements, blood in the stool, mucus and pus appear early. This discharge causes itching, burning and maceration of the skin around the anus. Neoplasms of this localization easily ulcerate due to their constant irritation by dense feces.
Due to the narrowing of the anus, the clinical picture of low intestinal obstruction develops. Common manifestations of rectal cancer include weakness, increased irritability, decreased appetite, decreased body weight, increased anemia, the appearance of low-grade fever, and increased erythrocyte sedimentation rate.
Symptoms of rectal sarcoma
Rectal sarcoma is quite rare. The group of rectal sarcomas usually includes the following tumors:
- Melanomas;
- Lymphosarcoma;
- Simple sarcomas;
- Hemangioendotheliomas.
The most common are melanoepitheliomas or melanomas. Melanoepithelioma, which was previously considered melanosarcoma, is localized in the anus, infiltrates the submucosal tissue and spreads upward to the intestine. The development of pigmented tumors near the anus is explained by the fact that in the embryonic period, elements of the epidermis penetrate into deeper tissues and serve as a source for the development of tumors.
Simple (round cell, spindle cell) sarcoma of the rectum is observed less frequently than melanoma, but more often than lymphosarcoma. Simple sarcomas develop from the submucosal layer of the intestine. They have the shape of a node the size of a pea to a fist, sometimes resembling a polyp on a wide base. The neoplasm most often originates from the anterior wall of the intestine and grows into the surrounding tissue. The mucous membrane above it retains its structure for a long time. Subsequently, it tightly fuses with the tumor and atrophies. A simple sarcoma does not metastasize to the lymph nodes for a long time, but metastases spread quite quickly through the blood vessels.
At first, patients feel awkwardness in the anus. Sometimes after defecation, pain occurs, which at times radiates to the perineum and sacrum. An increased urge to bottom may appear. As the tumor increases and the anus narrows or closes, abdominal pain and constipation occur, which are often replaced by diarrhea. Sometimes a dark liquid is released from the anus.
Heavy bleeding may occur, which patients and doctors perceive as hemorrhoidal. Bleeding is often the first symptom of colorectal cancer. Sometimes a tumor in the form of a pedunculated polyp falls out of the anus during defecation and is also easily reduced. Moderation of symptoms often does not cause concern for the patient.
During a digital examination of the rectum, a limited, mobile neoplasm is palpable. The tumor, even if it is significant in size, does not narrow, but only closes the intestinal lumen. The tumor may prolapse through the anus during straining and defecation. Most patients experience only a feeling of heaviness and pressure.
As the tumor grows, tenesmus occurs and signs of closure of the intestinal lumen appear. If the tumor ulcerates, bleeding occurs. The tumor, remaining limited for a long time, suddenly begins to metastasize to the inguinal and pelvic lymph nodes, distant organs (kidneys, liver, lungs, peritoneum). A local limited process turns into a general one. Sometimes, at the beginning of its development, sarcoma remains a mobile limited tumor for a considerable time, without penetrating deeper. This explains the importance of early diagnosis of this type of colorectal cancer.
Make an appointment
Symptoms and diagnosis of colorectal cancer in women
Signs of rectal cancer in women often appear at a late stage of cancer development, when the wall of the vagina and bladder is damaged. A fistula appears in the vagina, through which feces and gases escape. Rectal cancer manifests itself with symptoms similar to those of diseases of the stomach, intestines, and genitourinary system. Signs of rectal cancer at an early stage do not have any special manifestations; they are often similar to the manifestations of hemorrhoids and intestinal disorders.
Diagnosis of rectal cancer in women is carried out at the Yusupov Hospital using several methods:
- Endoscopic examination;
- Radiography;
- Ultrasound diagnostics;
- Computed tomography;
- Fibercolonoscopy;
- Radioisotope liver scan to detect metastases
The woman is examined by a gynecologist to rule out tumor growth in the uterus and vagina. If polyps or tumors of the rectum are detected, a biopsy is performed with histological examination of a tissue sample. An analysis is prescribed for tumor markers CA 19-9, carcinoembryonic antigen. Such studies are part of a comprehensive survey.
Symptoms in men
The first signs of rectal cancer in men, as in women, are intestinal discomfort, nausea, abdominal pain and the appearance of streaks of blood in the stool. As the tumor grows, the following symptoms appear:
- The appearance of pus in the stool;
- Persistent constipation that cannot be treated;
- Incontinence of feces and gases;
- Pain of varying intensity;
- A painful urge to defecate;
- Rumbling in the stomach and bloating.
When the tumor affects the lower part of the rectum and sphincter muscles, cancer symptoms appear at an early stage. The pain forces the patient to sit strictly on one buttock. When the tumor of the upper rectum grows into other organs and tissues, the pain intensifies. Over time, anemia, exhaustion, fatigue develops, and the skin becomes pale with a jaundiced tint. Rectal cancer often grows into the prostate gland and seminal vesicles. The size of the organ increases. The patient has difficulty urinating.