Esophageal cancer is a malignant disease arising from its mucous membrane. Cancer is the most common disease of the esophagus. Mostly men are affected (3:1); in women, esophageal cancer is not included in the list of the 10 most common cancers. Given the anatomical structure of the esophagus, the most common form of esophageal cancer in the world is squamous cell carcinoma .
In second place is esophageal adenocarcinoma , a cancer arising from the glandular epithelium.
Anatomy of the esophagus
The esophagus is a hollow muscular tube that connects the pharynx and oral cavity to the stomach. The wall of the esophagus is built from the mucous membrane, submucosa, muscular and adventitial membranes. The muscular lining of the esophagus consists of two layers: the outer longitudinal and the inner circular. In the upper part of the esophagus, the muscular layer is formed by transverse muscle fibers. At approximately the level of one third of the esophagus (counting from the top), striated muscle fibers are gradually replaced by smooth muscle fibers. In the lower part, the muscular layer consists only of smooth muscle tissue.
The mucous membrane is covered with stratified squamous epithelium; the submucosa contains mucous glands that open into the lumen of the organ.
In the esophagus there is a skin-type mucous membrane. The epithelium is multilayered squamous, non-keratinizing, lying on fine-fibrous connective tissue - its own layer of the mucous membrane, consisting of thin bundles of collagen fibers; also contains reticulin fibers and connective tissue cells. The own layer of the mucous membrane protrudes into the epithelium in the form of papillae.
A special feature of the esophagus is the absence of a serous membrane; the outer layer is represented by adventitia, loose connective tissue. Only in the lower third of the esophagus, more precisely its abdominal section, is covered with serosa.
Types of esophageal cancer according to the direction of tumor growth
Depending on where the tumor grows (into the lumen of the organ or deep into it), the following forms are distinguished:
- Endophytic (ulcerative).
- Exophytic (growing into the lumen of the esophageal tube).
- Sclerosing.
Endophytic cancer accounts for about 30% of all cases of esophageal cancer. This group includes scirrhus and ulcerative (saucer-shaped) cancer. Spreading circularly, such a tumor causes stenosis and spasm of the esophagus.
Exophytic esophageal cancer accounts for 60% of all cases. In this case, stenosis also develops, but it is caused by filling the lumen of the esophagus with tumor tissue. Exophytic forms include nodular, polyposis, fungiform, and medullary cancer.
The third form is scirrhous cancer, which is also called circular and infiltrative sclerosing.
Prevalence of esophageal cancer
Approximately 80% of all cases of esophageal cancer are diagnosed in developing countries , where the dominant histological form is squamous cell carcinoma. At the same time, adenocarcinoma, with rare exceptions, occurs only in industrialized countries.
The incidence of esophageal cancer is characterized by pronounced geographic variability with a 100-fold or more difference between the highest and lowest rates. The highest incidence (>150) was noted in Iran and other so-called countries. The Caspian belt, namely, in some areas of Turkmenistan and Kazakhstan adjacent to the Caspian Sea, as well as in Karakalpakstan, and in these regions endemic for esophageal cancer, the incidence is high both among men and among women. The incidence of esophageal cancer in the Muynak region of Karakalpakstan is 126 among men and 150 among women. Other areas of high incidence are some regions of China. High incidence has also been reported in Zimbabwe among black men (19). In developed countries, a relatively high incidence of esophageal cancer (>10) is reported in France (Calvados -17) and in the USA among black men (11).
In Russia, the incidence of esophageal cancer is relatively low and is comparable to similar indicators in other European countries. However, in some regions, for example in Yakutia, the incidence of esophageal cancer is much higher. A very high incidence of esophageal cancer (more than 150) is observed among the small peoples of the North and Far East of Russia. Mortality from esophageal cancer correlates with incidence rates and has the same geographic features.
The incidence of esophageal cancer is decreasing in most countries of the world, including Russia. However, in a number of developed countries in recent years there has been an increase in the incidence of adenocarcinoma of the cardiac esophagus, which, according to a number of cancer registries, accounts for more than 50% of all cases of esophageal cancer.
For esophageal cancer, the 5-year survival rate ranges from 5–12% and remains unchanged for two decades.
Causes and risk factors
The etiology of esophageal cancer has regional characteristics and also depends on the location and histological type of the tumor. The main risk factors for squamous cell carcinoma of the esophagus in developed countries are tobacco smoking and excessive consumption of alcoholic beverages. For adenocarcinoma of the cardia, along with these two factors, gastroesophageal reflux is important, which leads to constant irritation and damage to the mucous membrane of the cardia, its metaplasia and dysplasia.
The etiology of esophageal cancer in regions with very high incidence is not completely clear. Most likely, the very high risk of developing esophageal cancer in endemic regions, namely Iran, Central Asia and China, is associated with a deficiency of vegetables and fruits and, accordingly, vitamins and other microelements in the diet. In addition, the risk of developing esophageal cancer is believed to be increased due to the consumption of very hot drinks - tea in Iran and Central Asia and yerba mate in South America. There have been suggestions about the possible role of oral consumption of some forms of tobacco, such as betel nut, as well as opium. The role of HPV and food contamination with carcinogenic fungi is considered.
The development of squamous cell carcinoma of the esophagus is also associated with other diseases, such as:
- strictures (narrowing of the esophagus) due to the use of aggressive liquids or prolonged esophagogastric reflux,
- achalasia cardia,
- scleroderma,
- Plummer-Wilson syndrome (development of esophageal membranes in women with iron deficiency anemia).
In patients with a disease such as hyperkeratosis (palms and feet), which has an autosomal dominant type of inheritance, by the age of 45, squamous cell carcinoma of the esophagus develops in 50% of patients, and by 55 years – in 95%.
Esophageal cancer symptoms
Early forms of cancer are asymptomatic, since for difficulty swallowing food (dysphagia) to occur, a narrowing of the lumen of the esophagus of less than 15 mm is necessary.
Unfortunately, more than half of patients (60%) have an advanced stage of the disease at the time of diagnosis.
The main symptoms of esophageal cancer are:
- Dysphagia.
- Pain when swallowing food.
- Jumping off eaten food (regurgitation).
- Pain and discomfort in the chest.
- Feeling of a foreign body in the esophagus.
- Hoarseness of voice (if the recurrent laryngeal nerve is involved in the process).
- The appearance of enlarged lymph nodes in the neck.
- Loss of body weight.
Squamous cell carcinoma is characterized by the development of a locally widespread process involving adjacent vital anatomical structures, such as the aorta, trachea, main bronchi, and heart.
Metastasis of squamous cell carcinoma of the esophagus occurs through the lymphogenous route with the development of distant metastases in the liver, lungs, and bones.
Types of esophageal cancer depending on the external structure
Depending on the structure, the following types of esophageal cancer are distinguished:
- Scirrhus (fibrous, sclerosing). It appears in the form of a hardened area of the mucous membrane, grows circularly, causing a narrowing of the lumen of the esophagus, which is why it manifests itself early with spasms that are not relieved by antispasmodics. It ulcerates late; before this, only stenosis of the esophagus is detected during esophagoscopy; the biopsy is also negative, which often becomes the cause of diagnostic errors. Often, scirrhus is primarily formed in the stomach (see treatment of stomach cancer abroad) and then spreads to the esophagus, i.e., it is secondary.
- Brainy . It has the form of a soft formation, quickly spreads throughout the mucous membrane, and quickly disintegrates. Tumor formation is clinically manifested by moderate dysphagia (difficulty swallowing), which resolves after tumor disintegration, which can be misleading regarding the nature of dysphagia.
- Polypous . Outwardly, it resembles cauliflower inflorescences - multiple nodes of irregular shape. As polyps grow, they fill the lumen of the esophagus, causing dysphagia.
- Mushroom-shaped . Similar to polyposis, the only difference is that the outline is more regular, resembling a mushroom.
- Nodal . Unlike polypous and mushroom-shaped, it does not have a pronounced stalk.
- Saucer-shaped, or ulcerative . It is ring-shaped with clearly defined raised edges and an ulcerative formation in the center.
- Ulcerative . In this case, the cancerous tumor is not delimited from the neighboring tissue by roll-like edges, having a rounded shape, but looks uneven, capturing the neighboring tissue in the form of tongues or daggers.
In addition, esophageal cancer can be of a mixed form, for example, a polypous tumor, ulcerating, becomes saucer-shaped in a certain area.
Diagnostics
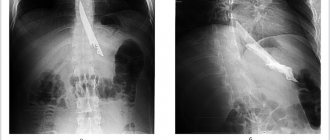
- The main diagnostic tools for patients with squamous cell carcinoma of the esophagus are barium radiography of the esophagus (detection of malignant stricture of the esophagus, its extent and the degree of narrowing of the esophagus) and endoscopic examination of the esophagus and stomach with a biopsy of the tumor.
- In order to establish the stage of the disease , exclude distant metastases and assess the local extent of the process, it is necessary to conduct MSCT of the chest and abdominal cavity with intravenous contrast.
- In order to assess the depth of tumor invasion, an endosonographic endoscopic examination is performed (simultaneous endoscopy and ultrasound).
- In patients with cancer of the middle third of the esophagus, fibrobronchoscopy to exclude involvement of the trachea and main bronchi in the tumor process .
- PET/CT (with 18F-deoxyglucose) is not very informative for determining the status of the primary tumor (T) and regional lymph nodes (N), but compared to CT it demonstrates higher sensitivity and specificity in detecting distant metastases; PET/CT is recommended if the patient does not have distant metastases according to CT.
Classification of esophageal cancer depending on cell differentiation
Cell differentiation is the acquisition by them during development of those characteristics that ensure their function and allow them to be classified as a particular tissue (for example, squamous or columnar epithelium).
Malignant or atypical cells are characterized by impaired maturation due to too rapid growth. Because of this, their differentiation is disrupted - these cells are not fully mature and are not able to fully perform their functions; instead, they begin to reproduce uncontrollably, which gives rise to a tumor. The less mature the cells, i.e., the less differentiated they are, the more aggressive the tumor behaves. Thus, well-differentiated tumors have a better prognosis, because they progress more slowly, metastasize later, and respond better to antitumor therapy. Poorly differentiated tumors leave little time for treatment because they grow quickly and metastasize quickly, which reduces the prognosis.
Depending on the degree of differentiation of tumor cells, the following types of esophageal cancer are distinguished:
- Highly differentiated - tumor cells have minimal differences from healthy ones (however, signs of atypia are present). It has the most favorable slow course, even developing for a long time, has single metastases, and is best treated.
- Moderately differentiated - an intermediate form characterized by average malignancy. If detected early, it has a fairly optimistic prognosis.
- Poorly differentiated . Tumor cells are characterized by polymorphism, that is, they are distinguished by an abnormal, unequal structure (they have a different number of nuclei, different sizes and shapes, the amount of cytoplasm, etc.). They have a tendency to rapidly divide and grow, and therefore have a high malignancy.
- Undifferentiated . The most aggressive type of tumor, most often develops secondarily in the esophagus. In this case, the reserved prognosis is further complicated by the presence of a primary tumor.
Classification
Squamous cell carcinoma of the esophagus, like all malignant tumors, is classified and staged in accordance with the international TNM classification (8th revision).
TNM Esophageal Cancer Staging System (UICC, 8th edition)
Primary tumor
Tx The primary tumor cannot be assessed;
T0 No evidence of a primary tumor;
Tis Carcinoma in situ/high grade dysplasia;
T1 Tumor growth into the lamina propria or submucosal layer;
T1a Tumor involves the lamina propria or lamina muscularis mucosa T1b Tumor invades the submucosal layer;
T2 Germination of the muscle layer;
T3 Germination of adventitia;
T4 Germination of adjacent structures;
T4a Pleura, peritoneum, pericardium, diaphragm, vein of azygos;
T4b Adjacent anatomical structures: aorta, vertebrae, or trachea.
Regional lymph nodes
Nx Regional lymph nodes cannot be assessed;
N0 No metastases in regional lymph nodes;
N1 Involvement of 1–2 regional lymph nodes;
N2 Involvement of 3–6 regional lymph nodes;
N3 Involvement of 7 or more regional lymph nodes.
Distant metastases
M0 No distant metastases;
M1 There are distant metastases.
The following groups of lymph nodes are regional:
- disgruntled;
- internal jugular;
- upper and lower cervical;
- cervical paraesophageal;
- pretracheal (bilateral);
- lymph nodes of the lung root (bilateral);
- upper paraesophageal (above v. azygos);
- bifurcation;
- lower paraesophageal (below v. azygos);
- posterior mediastinal;
- diaphragmatic;
- perigastric (right and left cardiac, lymph nodes, along the lesser curvature, along the greater curvature, suprapyloric, infrapyloric, lymph nodes along the left gastric artery).
Category pN0 can be established only after lymph node dissection with pathomorphological examination of at least 7 removed lymph nodes (in the absence of metastases in them).
Stages of cancer
Cancer tumors have 4 stages of development. Any stage reveals particular symptoms of the disease and methods of treatment. The stronger the damage, the brighter the symptoms, the more severe the disease is treatable.
It is worth considering the stage of cancer as it spreads:
- Stage 1 does not affect nearby organs. The location of the tumor is inside the esophagus. There are no metastases.
- Stage 2 affects the food channel, narrowing it. The tissue of the esophagus changes. Metastases are located on the lymph nodes.
- Stage 3 increases the damaged area by absorbing nearby organs. Metastases also form not only inside the esophagus, but also affect all organs located near the source of inflammation.
- Stage 4 closes the food canal, dysphagia appears. Metastases are distributed not only to nearby organs, but also affect distantly located organs.
This division is accepted by all doctors, who subsequently choose the method of diagnosis and further treatment for the patient.
Classification in the international system
The international TNM system determines the stages of a malignant tumor. This designation has an alphabetic and numerical abbreviation. Where T is the primary tumor; N – damage to regional lymph nodes; M – distant metastases; G – degree of differentiation according to Gleason.
To determine the primary tumor (T), the following numbers are used:
- Tis – data cannot be obtained, the neoplasm is pre-invasive.
- T1 – tumor size less than 2 cm, location – mucous and submucous membrane of the esophagus.
- T2 – tumor size more than 2 cm, lesions have reached the myometrium and muscular walls of the esophagus.
- T3 – all organs of the esophagus are affected, including the outer serosa.
- T4 – the spread of the tumor has reached its apogee: the diaphragm, aorta, pleura, trachea are damaged and the spine is affected.
To classify lesions of the lymph nodes, the following division is accepted:
- N0 – no damage.
- N1 – there are no more than two foci of malignant neoplasms in the lymph nodes.
- N2 – 3-6 areas damaged.
- N3 – tumor foci exceed 7.
For distant metastases, there are only two classifications, where M0 means no metastases, and M1 indicates their appearance.
Differentiation (G) is divided into G1 - highly differentiated; G2 – moderately differentiated; 3 – low differentiated.
Thus, stage 0 contains the abbreviation TisN0M0G1. Stage one: IA – T1N0M0G1, and IB – T1N0M0G2-3. Second stage: IIA – T1N0M0G2-3 or IIB – T2N1M0G2-3. Third stage: IIIA – T3N2M0G1-3 or IIIB – T3N3M0G1-3. The fourth stage of VIA is T4N0-3M1G1-3.
Stages of esophageal cancer
Esophageal cancer treatment
The main method of treatment is surgery. Only if surgical treatment is impossible (patient refusal or functional contraindications) is chemoradiotherapy performed independently.
If the tumor grows within the mucosa (T1), endoscopic resection within the mucosa or submucosa can be performed. Endoscopic resection is the method of choice for RP in situ and severe dysplasia. In addition, the method is successfully used for tumors of the esophagus that do not extend beyond the mucous membrane, in patients with a significant risk of surgical complications. At the same time, the 5-year survival rate reaches 85–100%.
Types of operations
- The main type of operation for RP is transthoracic subtotal resection of the esophagus with simultaneous intrapleural plastic surgery of the stomach stalk or a segment of the colon with bilateral two-zone mediastinal lymph node dissection from a combined laparotomy and right-side thoracotomy approaches (Lewis-type operation).
- If the tumor is localized in the upper thoracic or cervical regions, it is possible to perform transthoracic resection of the esophagus with anastomosis to the neck (McCain type operation).
- In some clinics, transhiatal resections of the esophagus are performed as an alternative, which cannot be considered radical. They should not be used in patients with thoracic esophageal cancer, since adequate mediastinal lymph node dissection above the tracheal bifurcation is not possible from the laparotomy approach.
- Another way to reduce the incidence of surgical complications is minimally invasive (thoraco-laparoscopic) or hybrid (thoracotomy + laparoscopy or thoracoscopy + laparotomy) esophagectomy or robot-assisted esophagectomy.
The choice of surgical treatment method for a tumor of the esophagogastric junction is determined by its localization according to the Siewert classification:
- in type I, a Lewis operation or a Garlock operation is performed depending on the size of the tumor, in exceptional cases (if thoracotomy is not possible) - transhiatal resection of the esophagus;
- in type II, transpleural proximal resection is performed (Garlock's operation) or transperitoneal proximal resection with a wide diaphragmotomy and high anastomosis in the mediastinum (in somatically aggravated patients);
- in type III, transperitoneal proximal resection or gastrectomy is performed.
For clinical stage II-III, treatment options are:
- preoperative chemotherapy + surgical treatment;
- preoperative chemoradiotherapy + surgical treatment;
- surgery;
- independent chemoradiotherapy.
Chemo and radiation therapy
The results of surgical treatment of RP at these stages remain unsatisfactory; only about 20% of patients survive 5 years. In order to improve treatment results, various combinations of drug and radiation therapy are used (preoperative chemotherapy, preoperative chemoradiotherapy, independent chemoradiotherapy).
In clinical stage IVa (T4 or multiple metastases in regional mediastinal lymph nodes), the main treatment method is independent chemoradiotherapy. However, involvement of the pericardium, pleura, lung and diaphragm does not exclude the possibility of surgical treatment in case of an objective response to preoperative therapy.
The main goals of treatment of patients with cancer with distant metastases are to improve the quality of life by eliminating symptoms caused by tumor growth and increasing life expectancy. Assessing the effectiveness of various chemotherapy regimens in this category of patients is difficult due to the lack of randomized studies, especially for squamous cell carcinoma. For the same reason, it is difficult to assess the benefit that chemotherapy provides compared to symptomatic therapy.
Chemotherapy is recommended for patients in satisfactory general condition (ECOG score 0–2 points) in the absence of severe (grade III–IV) dysphagia that makes it difficult for the patient to adequately feed. In the latter case, the first stage shows restoration of esophageal patency (stenting, recanalization). For grade I–II dysphagia, chemotherapy can reduce its severity in a number of patients by the end of the first course.
The most effective drugs for both histological variants are cisplatin, fluoropyrimidines, and taxanes.
For squamous cell carcinomas, the standard chemotherapy regimen remains a combination of cisplatin with an infusion of 5-fluorouracil or capecitabine; the rate of objective effects when using such regimens is about 35%, and life expectancy does not exceed 6–8 months. Carboplatin is inferior to cisplatin in terms of immediate effectiveness, which limits its use outside chemoradiotherapy programs.
The use of taxanes is possible as part of two-component regimens with cisplatin or three-component combinations (with cisplatin and fluoropyrimidines). In the latter case, at the cost of greater toxicity, it is possible to increase the objective effect to 48%, but this apparently does not lead to an increase in life expectancy.
Reviews from our patients
- Review of the treatment of obstructive jaundice
Review of the treatment of obstructive jaundice April 9, 2021The patient was admitted with severe signs of jaundice. During hospitalization, his condition stabilized. For this purpose, drainage of the bile ducts was carried out, as well as exposure to medications. After receiving the results of the histochemical study, further treatment tactics will be determined.
read more
- “They have golden hands”...
“They have golden hands”... April 7, 2021
Patients are being treated at the Medicine 24/7 clinic. During the treatment, they managed to become friends and this time decided to record a joint review. They thank all the clinic staff for the high organization of all processes and the effectiveness of the procedures.
read more
- Chemotherapy - review by Olga Stepanovna
Chemotherapy - review by Olga Stepanovna April 6, 2021
The patient is hospitalized for the third time. During a comprehensive examination, a puncture of the tumor was performed. Histological analysis made it possible to verify the diagnosis and determine treatment tactics. At the first stage of treatment, surgery was performed. The tumor was radically removed. Drug treatment is now being carried out to prevent the possibility of relapses. To date, the first course of chemotherapy has been completed. The patient was discharged home in satisfactory condition.
read more
- “You are the only clinical organization that brings benefits to people”...
“You are the only clinical organization that brings value to people”... April 6, 2021
The patient was admitted for treatment of cancer. The hospitalization lasted a week. The patient notes that they immediately responded to all his problems and provided assistance in a timely manner. He compares the Medicine 24/7 clinic with other medical institutions. Patient o...
read more
- Review of the attending physician M.Kh. Mustafaeva
Review of the attending physician M.Kh. Mustafaeva April 2, 2021
The patient was hospitalized in serious condition. Complex treatment was carried out. A positive effect has been achieved. The patient’s wife thanks her husband’s attending physician Milana Khanlarovna Mustafaeva. She says: “From the first day, from the first minute, as soon as we came to you, we immediately felt and understood each other. You understood the patient, you understood me. You have defined to the depth of the volume that we need. Although I couldn't explain how...
read more
- Feedback on the treatment of breast disease
Feedback on the treatment of breast disease April 1, 2021
The patient was hospitalized with breast disease. By decision of the council, surgery was performed at the first stage of treatment. It was successful. On the third day the patient was discharged home. After histological examination, further treatment tactics will be determined.
read more
- Feedback on the treatment of ascites
Review of the treatment of ascites March 30, 2021
The patient contacted the Medicine 24/7 clinic for treatment of ascites and pleurisy. These conditions are characterized by abnormal accumulation of fluid in the abdominal and pleural cavities, respectively. This happens with cancer. A laparocentesis procedure was performed, during which the fluid was evacuated. The patient's condition improved markedly.
read more
Radiation therapy
Radiation therapy is often combined with chemotherapy and surgery. It may also be prescribed before, after surgery, or in later stages as the primary treatment.
In addition to radiation from external sources, brachytherapy can be performed - a procedure during which a miniature radiation source is placed directly next to the tumor for a while. This method is usually used in later stages to make swallowing easier.
Targeted therapy
Targeted drugs are a modern class of drugs directed against specific target molecules in tumor cells. For inoperable esophageal cancer, two targeted drugs are used:
- Trastuzumab (Herceptin) blocks HER2, a receptor protein that is found on the surface of cancer cells and promotes their rapid proliferation. The drug is administered intravenously once every 3 weeks, usually in combination with chemotherapy.
- Ramucirumab (Cyramza) blocks VEGF, a molecule that cancer cells use to stimulate the growth of new blood vessels. It is administered intravenously once every two weeks.
In order for targeted drugs to have their effect, the appropriate target molecules must be present in cancer cells. In order to check this, a biopsy is performed and the material is sent for molecular genetic analysis.
Immunotherapy
Immunotherapy drugs help the immune system recognize and destroy tumor cells. For esophageal cancer, the immune drug pembrolizumab (Keytruda) from the group of checkpoint inhibitors is used in some cases. It blocks the PD-1 protein, which suppresses the immune response. Thus, the immune system is activated and begins to attack the tumor tissue.
Pembrolizumab is prescribed after at least two treatment regimens with other anticancer drugs have been tried. Keytruda is administered intravenously every three weeks. This helps slow the growth of the tumor or reduce its size.
Leave your phone number
we will definitely call you back
Palliative treatment
The most common symptom of RP is dysphagia. The need to eliminate it may arise at all stages of treatment. Various methods are used to eliminate dysphagia:
- endoscopic procedures (balloon dilatation, electro-, argon plasma or laser destruction, photodynamic therapy),
- radiation therapy (external beam or brachytherapy),
- placement of intraluminal stents.
Endoscopic procedures provide a quick but short-term effect and are suitable in cases where treatment with expected high effectiveness (surgical, medicinal, radiation) will be started in the near future.
In cases where curing the patient is impossible, the optimal options for correcting dysphagia are brachytherapy, esophageal stenting, or external beam radiation therapy.
Palliative chemoradiation therapy has no clear advantages compared to RT (without chemotherapy) and is associated with greater toxicity. According to the results of the study, esophageal stenting allows for faster achievement of the desired effects, however, with a longer observation period compared with brachytherapy, the frequency of complications (stent migration, pain, perforation, gastroesophageal reflux) was higher, and the frequency of complete relief of dysphagia was slightly lower. With the development of esophageal-bronchial or mediastinal fistulas, the placement of covered stents can stop these complications in 70–100% of patients.
Observation
Active surveillance is indicated for patients for early detection of relapse in the esophagus for the purpose of surgical intervention or relapse in the mediastinum for the purpose of chemoradiotherapy. The scope of the examination depends on the stage of the disease and previous treatment:
Stage I (after endoscopic mucosal/submucosal resections) and stages II–III (after chemoradiotherapy, with prospect of esophagectomy in case of recurrence):
- EGDS – every 3–4 months. during the first two years, every 6 months. – during the third year, then annually until the total observation period is 5 years.
- CT scan of the chest and abdominal organs – every 6 months. during the first 2 years, then annually until a total observation period of 5 years;
Stage I–III (after surgical treatment):
- CT scan of the chest and abdominal organs – every 6 months. during the first 2 years, then annually until a total duration of 5 years.
Other examination methods are recommended for other categories of patients if clinically indicated. Performing PET/CT and determination of serum markers for monitoring patients is not recommended.
Screening: can esophageal cancer be detected in the early stages?
Screening is currently only recommended for those at high risk of developing esophageal cancer, such as patients with Barrett's esophagus. Periodic endoscopic examinations are carried out, and a biopsy may be performed if indicated.
In some cases, prophylactic treatment is recommended for Barrett's esophagus when there is a very high risk of malignancy. Resection of the esophagus, endoscopic resection of the mucous membrane, radiofrequency ablation, and photodynamic therapy are performed.
Surgical treatment in the department of thoracoabdominal surgery and oncology of the Russian Scientific Center for Surgery
Treatment in the department is carried out under the programs of compulsory medical insurance, voluntary medical insurance, VMP, as well as on a commercial basis. Read how to get treatment at the Department of Thoracoabdominal Surgery and Oncology of the Russian Scientific Center for Surgery.
To schedule a consultation, call:
+7 (499) 248 13 91 +7 (903) 728 24 52 +7 (499) 248 15 55
Submit a request for a consultation by filling out the form on our website and attaching the necessary documents.
Survival prognosis
The prognosis for esophageal cancer depends on the stage. The 5-year survival rate (proportion of patients alive 5 years after diagnosis) at different stages is:
- Tumor limited to the wall of the esophagus: 45%.
- Tumor that has grown into adjacent tissue or spread to lymph nodes: 24%.
- Cancer with metastases: 5%.
With inoperable cancer in the later stages, it is impossible to cure the patient, but doctors can prolong his life, improve his general condition, and relieve painful symptoms. The Medicine 24/7 clinic accepts patients with malignant tumors at different stages. Our doctors know how to help you. Sign up for a consultation by phone: +7 (495) 230-00-01.
The material was prepared by oncologist, thoraco-abdominal surgeon, head of the department of surgery at the Medicine 24/7 clinic, Alexander Valerievich Korotaev.