Adenocarcinoma in the intestine is formed from mutated glandular epithelial cells that have lost, to one degree or another, their differentiation (that is, their normally inherent structural characteristics) and began to divide and spread uncontrollably throughout the body.
Adenocarcinoma of the colon is one of the most common types of cancer; malignant tumors of the small intestine are much less common. The initial symptoms of intestinal adenocarcinoma, like most malignant tumors, are nonspecific, and almost never alert or prompt the patient to see a doctor, which significantly worsens the prognosis. Moreover, very often a tumor develops against the background of an already existing chronic intestinal pathology, and its symptoms are mistaken for an exacerbation of an already known disease.
What is adenocarcinoma?
Adenocarcinoma (glandular cancer) is a malignant tumor that is formed from glandular epithelium. Glandular cells are present in all organs of external and internal secretion. Glandulocytes have exactly the same characteristics as ordinary epithelium, but are also capable of releasing their secretions into the external environment (intestinal lumen) or into the blood directly. They are found in the glands of the skin, salivary glands, stomach and intestines, pancreas, etc. Under the influence of unfavorable factors, they malignize into adenocarcinoma.
It turns out that adenocarcinoma can develop in any organ where there are glands. During the development of the disease, the tumor grows into the lumen of the gastrointestinal tract, can affect nearby organs and gives distant metastases. Adenocarcinomas may not lose the ability to produce secretory fluid, which contains various substances, and therefore, serous and mucosecretory tumors are distinguished. The neoplasm can have various shapes and sizes.
Histological types of colon adenomas
There are 3 histological types of colon adenomas:
- Tubular;
- Tubular villous;
- Villous.
The separation criterion is the ratio of villous and tubular structures. Tubular adenoma of the colon - what is it? Microscopically, tubular adenoma is represented by proliferating adenomatous epithelium. The tumor consists of branching and significantly convoluted glandular tubes, longer than in the normal intestinal mucosa. In tubular adenoma, no more than 25% villous tissue is present. Tubular adenoma of the colon has a mucous membrane-covered base. It is represented by connective tissue, smooth muscle cells and blood vessels. Tubular adenomas have a stalk and a smooth lobulated surface. Less often they are located on a wide base. Creeping tubular adenomas, which protrude slightly above the surface of the mucous membrane, are very rare.
In tubular-villous adenomas, the number of villi increases, which can be detected both on the surface of the polyp and inside large glands. The glands lengthen, acquire an irregular shape, and fit tightly to each other. The degree of epithelial dysplasia increases. In tubular-villous adenoma, the percentage of villous tissue varies from 25 to 75%. The tumor consists of pronounced lobules and has small areas with villi or very small lobules.
Villous adenoma consists of thin finger-like outgrowths of the connective tissue of the lamina propria, which are covered with epithelium. In villous adenomas, a small number of glands and 75% of the villous component can be found. Macroscopically, villous adenomas have a wide base and a “shaggy” surface. There is a special histological type of colon adenoma - serrated adenoma. The tumor is close in structure to a hyperplastic polyp, but has the potential for malignancy.
Adenomatous epithelium belongs to the category of neoplastic. For this reason, each adenoma has signs of dysplasia of varying severity. Histologists distinguish 3 degrees of dysplasia of tubular adenoma of the colon:
- 1st degree – weak;
- 2 degrees – moderate;
- Grade 3 – severe.
Tubular adenoma of the colon with low grade dysplasia is a poorly differentiated tumor. It can transform into adenocarcinoma.
Causes
According to statistics, most cases of the development of malignant tumors are associated with disruption of the functioning of glandular cells and disruption of the outflow of secretions. Adenocarcinoma can be provoked by eating large amounts of smoked meats, sweets, fatty and floury foods in the daily diet.
There are general and specific factors that provoke this disease.
Common reasons include the following:
- Heredity.
- Poor nutrition.
- Failures in genetics.
- Chronic diseases.
- Large doses of radioactive radiation.
- Working with toxic materials.
- Smoking.
- Papilloma virus.
Specific factors that provoke cell mutation:
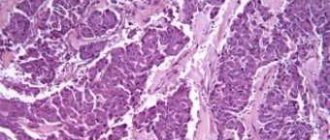
Illustration - adenocarcinoma
- Adenocarcinoma often develops in the intestines due to fistulas, regular constipation, chronic colitis, and polyps of the mucous membrane.
- Hot food can cause burns in the esophagus, which leads to adenocarcinoma.
- Glandular cancer can form against the background of a long-term inflammatory or autoimmune disease.
- It can occur in the liver after viral hepatitis, against the background of cirrhosis.
What does colon cancer look like?
Doctors at the Yusupov Hospital collect material from a rectal tumor during an endoscopic examination or surgery and send it to the histology laboratory. Laboratory assistants determine the histological type of the tumor based on what colorectal cancer looks like.
Rectal adenocarcinoma consists of atypical cells that originate from glandular epithelial tissue and are formed into tubular, papillary and other structures. The cellular structure can have varying degrees of differentiation: highly differentiated neoplasms have cytological signs of maternal epithelial tissue, and poorly differentiated adenocarcinomas only vaguely resemble the original material. They are highly aggressive, grow and spread faster.
Mucous adenocarcinoma is a group of cells that are surrounded by mucus. Tumors of the mucous type can be poorly differentiated and highly differentiated. Mucus accumulates in tumor structures in the form of “lakes” of varying sizes
Signet ring cell carcinoma gets its name due to the shape of the cells, which, due to an excess of mucus in them and the displacement of nuclei towards the membranes, take on the appearance of a ring. The mucous substance that occupies the space of cells is a specific protein mucin. Signet ring cell tumors of the rectum are quite aggressive.
Squamous cell carcinoma of the rectum consists of atypical cells. They belong to the squamous intestinal epithelium. Pathological lesions contain intercellular bridges and keratin. Rectal squamous cell tumors can be keratinizing or non-keratinizing.
Glandular squamous adenocarcinoma is a rare type of rectal cancer. Such neoplasms are represented by adenocarcinoma, in combination with squamous cell carcinoma. Under a microscope, histologists see small fragments of squamous cell transformation.
Undifferentiated rectal tumors consist of atypical cells of epithelial tissue that do not form glandular structures and do not produce mucus. These cells represent different cytological structures. They form sheets or cords that are separated by a scant stroma of connective tissue.
Scirrhus is a cancerous tumor in which the connective tissue predominates over the stroma. Cytological structures in scirra are cubic cells collected in strands or small cells. Sometimes there are neoplasms in the rectum that do not fit into any histological type. In this case, oncologists talk about unclassified rectal cancer.
Neuroendocrine tumors of the rectum originate from cells of the diffuse neuroendocrine system. They have a well-developed fibrous stroma and are histologically different from adenocarcinomas.
Symptoms of adenocarcinoma
The course of adenocarcinoma has three stages:
- Latent, it is also called hidden due to the absence of any symptoms.
- The period when the first symptoms appear, as the tumor grows, they intensify: pain in the tumor growth area, constipation, the appearance of blood clots, enlarged lymph nodes.
- Clear signs of damage to one or another organ due to the intensive growth of cancer cells, tumor disintegration, the appearance of metastases, cancer ulcers, intestinal obstruction, etc.
The patient does not show any symptoms for quite a long period.
As the tumor grows, nonspecific manifestations begin to appear, including: weight loss, decreased hemoglobin, sleep disturbance, fatigue, and decreased level of work ability.
When adenocarcinoma forms in the intestine, the following symptoms occur:
- abdominal pain;
- nausea, vomiting;
- intestinal obstruction;
- discomfort after eating;
- the presence of mucus and bloody discharge in the stool;
- alternating constipation with loose stools.
Localization of adenocarcinoma in the esophagus:
- difficulty swallowing (dysphagia);
- pain when swallowing (odynophagia);
- severe drooling as a result of narrowing of the esophagus.
Adenocarcinoma of the pharynx or nasal cavity is characterized by the following symptoms:
- pain in the nose, pharynx and larynx;
- chronic inflammation and swelling of the tonsils;
- pain when swallowing, which spreads to the ears and can also impair speech;
- enlarged lymph nodes or salivary glands.
Symptoms of liver adenocarcinoma
- feeling of pain in the right hypochondrium;
- accumulation of fluid in the abdomen;
- yellow tint to skin and eyes.
Symptoms of moderately differentiated adenocarcinoma
Specific signs depend on the location of the cancer focus. At first, this type of lesion is asymptomatic or there are general pathological signs. The list of such signs includes: weight loss caused by lack of appetite, weakness, decreased ability to work, excessive irritability, constant feeling of anxiety, depression, drowsiness or, conversely, insomnia, pain in the lower abdomen and epigastrium, pale skin, swelling, systematic fevers , presence of foreign substances in feces and urine, cough, periodic occurrence of shortness of breath; Signs of intoxication may be present. At the stages of spread of the oncological process to nearby and distant organs, these symptoms intensify; Also, specific symptoms appear, the lymph nodes become enlarged.
Diagnosis of adenocarcinoma
Banal laboratory tests allow one to suspect oncology based on an increased ESR, changes in the leukocyte formula, or a low red blood cell count. Detection of traces of blood in the stool allows one to suspect a malignant process. But it can easily be confused with a bleeding ulcer. Therefore, an accurate diagnosis can be established only on the basis of histological examination of the biopsy specimen.
To establish the exact size of the tumor, the degree of invasion into the wall and nearby organs, and to identify or exclude metastases, it is necessary to examine patients using PET, CT, and ultrasound.
Fluoroscopy allows you to determine the shape, exact location of the tumor and possible complications. To do this, contrast agents are used. Barium is often used in gastroenterology.
An endoscope is used to visually examine internal organs to confirm or rule out disease. During an endoscopy, a biopsy may be performed to examine the tissue under a microscope.
Diagnosis of pathology
To detect the oncology in question, the following procedures are performed:
• blood test; • histological examination of biomaterial removed by biopsy; • MRI; • CT; • PET; • angiography; • endoscopic type procedures (gastroscopy, bronchoscopy).
Thanks to these diagnostic measures, it is possible to identify the stage of progression of the oncological process and the extent of cancer spread throughout the body. In addition, with their help it is possible to prescribe the most adequate treatment.
Treatment of adenocarcinoma
Surgery
The main type of treatment for adenocarcinoma abroad is surgery in combination with a course of chemotherapy and radiation therapy. Radical tumor removal significantly increases the chances of recovery. In Israel and Germany today there are various pharmacological agents that contribute to the effectiveness of radical surgery.
Tomotherapy
This is an innovative method of radiation therapy in the treatment of adenocarcinomas. The 3-D scanner used during treatment accurately identifies the area affected by cancer and allows precise exposure of the tumor with high-frequency rays, practically without affecting healthy tissue. Thus, doctors can easily select the optimal radiation dose, scheme, and determine the exact irradiation zone with minimal harmful effects on healthy tissue. This technique is most often used to treat cancer of the esophagus and lungs.
Radiation therapy
Radiotherapy is effective in reducing pain after surgery, for tumors that cannot be completely removed or for inoperable metastases. More often, radiation therapy is used as an additional method to complex treatment.
Chemotherapy
Chemotherapy after surgery significantly improves the prognosis for life. The course of treatment is purely individual. Chemotherapy is used as an independent treatment method in cases where the tumor is inoperable, as well as during relapses to prolong the patient’s life and improve well-being.
Oncology centers abroad are equipped with the latest equipment, and the oncology specialists working there use the latest techniques for treating adenocarcinomas. For free information about cancer treatment abroad, please contact us and we can provide you with detailed information as soon as possible.
Forecasts and preventive measures
Survival prognosis is highly dependent on the stage of progression of the cancer process and the location of the lesion. If we talk about the initial stages of development of moderately differentiated adenocarcinoma of the large intestine, uterus and stomach, then the prognosis (provided that the operation is performed well) is quite good. According to statistics, everything ends well for 90% of patients. If the pancreas is damaged, the prognosis worsens. In people with damage to the lymphatic system, survival rates drop to 60%. If metastasis occurs, then the chances of crossing the 5-year survival threshold are 10-20%.
Results:
Of the 5489 patients, 136 (2.5%) and 155 (2.8%) were diagnosed with low-grade adenocarcinoma or mucinous colon cancer, respectively, by pathological examination. Identification of low-grade adenocarcinoma was associated with a poorer prognosis than in other groups (HR, 1.69, 95% CI 1.00-2.87, p = 0.051), especially in the subgroup of patients who received adjuvant chemotherapy (HR 2 ,16). Although mucinous tumors had an intermediate effect on outcomes in patients with stages I-III (RR, 1.33; 95% CI, 0.90-1.96), they were found to be an independent prognostic factor in patients with Stage II, which is associated with a higher rate of local relapses.
The difference between hemorrhoids and rectal cancer
Hemorrhoids and rectal cancer are proctological diseases that occur most often. How to distinguish hemorrhoids from colorectal cancer? You can independently determine the nature of the disease by the symptoms, but it is best to seek advice from the doctors at the Yusupov Hospital. Oncologists will conduct a comprehensive examination and differential diagnosis.
Hemorrhoids and rectal cancer have very similar symptoms and are well camouflaged. For a long period of time they do not manifest themselves in any way. A characteristic difference is the color of the blood. With hemorrhoidal bleeding, the blood is bright scarlet in color and practically does not mix with the feces. In cases of colorectal cancer, dark blood appears during bowel movements. It is evenly distributed in the feces.
Cancer and hemorrhoids are manifested by characteristic discharge. With pathological inflammation of hemorrhoidal veins, the mucus is transparent and does not have a pungent odor. A sign of rectal cancer is the presence of a foul-smelling, purulent substance in the stool, which appears not only during bowel movements.
With hemorrhoids, stool does not change shape. The growth of a malignant tumor, the gradual narrowing of the lumen of the anus contributes to the formation of ribbon-like feces. With hemorrhoids, patients deliberately refuse to eat because of pain during constipation or bowel movements, while they experience hunger and lethargy. With rectal cancer, the patient does not complain of poor appetite, but rapidly loses body weight.