Causes
The causes of colon ulcers may differ in different parts of the intestine.
All etiological factors are conventionally divided into major and minor.
Main reasons
The main causes of colon ulcers are associated with mechanical effects on the mucous membrane or inflammatory processes.
These include:
- Chronic constipation and injury to the mucous membrane from fecal stones.
- Mechanical injuries of the colon and rectum (in particular, when trying to free the rectum with your fingers from feces).
- Prolapse (prolapse) of the rectum or intussusception of the overlying sections of the large intestine into the lower sections.
- Chronic inflammatory processes in the large intestine.
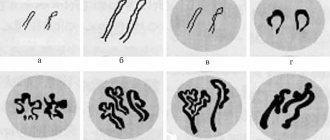
As a result of prolapse, ischemia of the colon wall develops and single or multiple ulcers are formed.
Secondary reasons
In addition to mechanical injuries, other possible causes of ulcerative defects in the large intestine have been identified:
- hereditary predisposition;
- radiation therapy of the pelvic organs;
- chronic intestinal infections and previously suffered severe infectious diseases;
- taking certain medications - anti-inflammatory, steroid hormones and others.
Less commonly, the cause of the disease is autoimmune inflammatory processes.
Risk factors
Doctors have identified negative factors that increase the risk of developing colon ulcers.
These include:
- chronic intoxication;
- bad habits and chemical addictions;
- poor nutrition, abuse of fatty, spicy and salty foods;
- stress and depression.
Symptoms of colon ulcers in adults can be provoked by chronic kidney and heart diseases, accompanied by organ failure.
Clinical manifestations of colon ulcers
An ulcer of the large intestine is manifested by specific local symptoms and general reactions of the body. The greatest severity of clinical manifestations occurs during the period of exacerbation of the disease. In addition, symptoms depend on the stage of development of the pathology.
Symptoms of colon ulcers in the early stages of the disease
In the initial stages, the disease is asymptomatic. As it progresses, symptoms of a colon ulcer appear, similar to an inflammatory process in the intestine.
These include:
- abdominal pain;
- bloating (flatulence);
- stool disorder.
When the rectum is affected, there is usually a feeling of incomplete bowel movement.
Classification
In practical medicine, several classifications of colon ulcers are used, corresponding to different criteria.
According to the speed of development and course, the defect can be:
- sharp;
- chronic recurrent;
- chronic without remission or continuous.
Based on the number of defects there are:
- single (solitary);
- multiple ulcers.
By localization they distinguish:
- total damage to the large intestine;
- left-sided ulcers;
- distal ulcers arising in the sigmoid or rectum.
In addition, ulcerative defects can be complicated or uncomplicated.
Intestinal manifestations
Local symptoms of colon ulcers are caused directly by irritation of the mucous membrane.
These include peristalsis disorders, pain syndrome, and pathological discharge from the rectum.
Constipation, diarrhea
A characteristic sign of damage to the large intestine is unstable stool with alternating constipation and diarrhea. More often, patients complain of constipation - the absence of stool for several days. The stool is hard. In severe cases, fecal stones and intestinal obstruction are formed.
After visiting the toilet, the feeling of bowel movement does not come, the patient experiences discomfort. Diarrhea occurs during the period of exacerbation of the ulcer. Stools are frequent and scanty, mixed with blood or mucus.
Appearance of pain
Pain from an intestinal ulcer most often occurs in the lateral areas of the abdomen or in the anus. If the transverse colon is affected, discomfort may occur above the navel or in the epigastric region, simulating the symptoms of gastritis.
The nature of the pain is:
- acute cramping;
- cutting;
- dull bursting.
Symptoms are usually not associated with food intake, but may worsen after eating milk, cereals or vegetables. The pain decreases after visiting the toilet and passing gas.
Discharge of blood during bowel movements
A common symptom of colon ulcers is bloody discharge in the stool. The closer to the anus the ulcer is located, the less altered the blood in the stool is.
When bleeding from the proximal colon, the blood is altered by the action of digestive enzymes. Stool takes on a tarry appearance, as when bleeding from the stomach or duodenum (melena).
Fresh (scarlet) blood appears in the stool with an ulcer of the rectum or sigmoid colon.
Extraintestinal manifestations
Extraintestinal symptoms are caused by the impact of pathology on the entire body.
These include:
- Anemia caused by chronic blood loss.
- Symptoms of general intoxication are weakness, malaise, headache, nausea.
- Astheno-neurotic syndrome caused by chronic pain.
Patients often lose weight, sleep poorly, become tearful and irritable, which indicates the negative effect of colon ulcers on the nervous system.
Anemia
With a colon ulcer, hypochromic iron deficiency anemia develops. It is caused by acute or chronic blood loss.
Signs of iron deficiency anemia are:
- pallor of the skin and visible mucous membranes;
- dry skin, brittle hair and nails;
- increased fatigue, weakness;
- frequent dizziness and fainting.
A characteristic symptom may be a violation of taste preferences - the desire to eat chalk, toothpaste and other inedible substances.
Dangerous symptoms of a colon ulcer
Symptoms of a complicated ulcer are considered prognostically unfavorable.
These include:
- an admixture of fresh blood in the stool is a sign of intestinal bleeding;
- acute (stabbing) or diffuse pain in the abdomen - a sign of perforation of the ulcer and the development of peritonitis (inflammation of the peritoneum);
- an increase in body temperature is a sign of an inflammatory process.
A sharp weight loss and the appearance of symptoms of intoxication are considered unfavorable. They indicate the possible degeneration of the ulcer into a malignant tumor (cancer).
Complications and risks
Complications of a colon ulcer pose a danger to the sick person.
These include:
- bleeding from affected intestinal vessels;
- perforation (perforation) – a through breakthrough of the intestinal wall;
- toxic dilatation (megacolon) – the colon stops contracting, gases and feces accumulate in it, which leads to severe intoxication;
- malignancy of the ulcer – cancerous degeneration;
With cicatricial narrowing of the intestinal lumen, intestinal obstruction often develops.
How to identify a colon ulcer yourself
The patient will not be able to make an accurate diagnosis on his own. However, based on characteristic clinical signs, you can suspect intestinal damage in order to consult a doctor in time and undergo an examination.
Symptoms to watch out for:
- pain in the lower abdomen or tailbone area;
- lack of feeling of bowel movement after visiting the toilet;
- bleeding during bowel movements.
The symptoms of an ulcer are similar to other, more serious diseases, so in no case should you self-medicate.
Perforated stomach ulcer
The goal of therapy for a perforated gastric ulcer is not only to save the patient’s life and eliminate the defect in the stomach wall, but also to treat gastric ulcers and general peritonitis. In the practice of a gastroenterologist and surgeon, there are cases of conservative management of a perforated gastric ulcer. Conservative treatment is used only in two cases: with decompensated somatic pathology and the patient’s categorical refusal to undergo surgery. Conditions for conservative treatment: less than twelve hours from perforation, age no more than 70 years, absence of tension pneumoperitoneum, stable hemodynamics. The complex of conservative treatment includes pain relief, administration of antibiotics and antisecretory drugs, anti-Helicobacter and detoxification therapy.
In the surgical treatment of perforated gastric ulcers, there are three main approaches: closure of the perforation, excision of the gastric ulcer, and gastric resection. In most patients, the perforation is closed by tamponade, covering with an omentum, or suturing. Indications for closure of a perforated gastric ulcer: asymptomatic perforation, disease duration of more than 12 hours, presence of signs of peritonitis, extremely serious condition of the patient. Starting treatment later than 24 hours after perforation triples mortality. Anti-Helicobacter and antisecretory therapy in the postoperative period can improve the results of surgery to close the perforation.
Excision of a perforated gastric ulcer is performed only in every tenth patient. This operation is indicated in the presence of gastric stenosis, bleeding, ulcers with callous edges, large perforations, and suspected malignancy of the ulcer (excision is necessary for pathomorphological examination).
Gastric resection can be performed in patients with a perforated ulcer if it is impossible to perform a simpler operation and carry out postoperative anti-Helicobacter and antisecretory therapy. Typically, such indications arise in the case of a complicated course of a peptic ulcer (peptic, penetrating and peptic ulcers; multiple ulcers), suspicion of a malignant process, repeated perforation of a gastric ulcer, or a huge size of the perforation hole (more than 2 cm).
In approximately 10% of patients, minimally invasive surgical techniques are used: laparoscopic and endoscopic treatment of gastric ulcers. The use of laparoscopic operations can significantly reduce the incidence of postoperative complications and mortality. Various surgical techniques can be combined with each other (for example, laparoscopic with endoscopic) and with vagotomy (selective proximal vagotomy, truncal vagotomy, endoscopic vagotomy).
If vagotomy was not performed during the operation, antiulcer therapy (proton pump inhibitors and H2-histamine receptor blockers, anti-Helicobacter drugs) is prescribed in the postoperative period.
Diagnostic features
Diagnosis of the disease begins with questioning and examining the patient, and carefully collecting anamnesis. Based on the data obtained, the doctor makes a preliminary diagnosis. Laboratory and instrumental examination methods help confirm it.
Data collection and inspection
During the first examination, the doctor examines the patient’s complaints, clarifies their nature, time of occurrence, connection with external factors (eating disorders, stress, physical activity, etc.). Then he clarifies the family history of the disease, correlates the social status, lifestyle and living conditions of the patient with the occurrence of symptoms. Particular attention is paid to diseases of the digestive tract in the patient's family.
Upon examination, decreased nutrition and pallor of the skin are revealed. Palpation (palpation) of the anterior abdominal wall determines pain along the large intestine or in the lower abdomen. Digital examination of the rectum is informative if the ulcer is located in the lower sections.
Laboratory research
Laboratory blood tests reflect general changes in the body caused by an ulcer, as well as specific signs of pathology. In the general blood test, hemoglobin levels were reduced. Most often they are caused by blood loss.
When an inflammatory process occurs, the ESR and the number of leukocytes increase. These changes are nonspecific for intestinal ulcers and are taken into account in conjunction with the results of other studies.
More accurate information is provided by a coprogram - a stool examination. The sample of biological material contains impurities of blood and mucus. The condition of the red blood cells found in the stool allows us to judge the height of the lesion. When bleeding from the rectum, traces of fresh blood are found.
If the ulcer is located in the colon, the blood is darker, reminiscent of gastric bleeding (tarry stool - melena). Stool analysis detects helminth and protozoan eggs if the patient is infected with these parasites.
The study is valuable for differential diagnosis with amebiasis and other diseases with a similar clinical picture.
Diagnostic procedures
Instrumental diagnostic methods make it possible to identify the nature of intestinal damage and its exact location.
On the eve of the examination, you must adhere to a special diet for several days. The intestines are thoroughly cleaned before the procedure.
Irrigoscopy
This is a method of x-ray examination of the large intestine using a contrast agent. Barium sulfate is injected into the patient's rectum and an image is taken.
The method evaluates:
- Elasticity of the intestinal wall, lumen width, possible cicatricial narrowings.
- Relief of the mucous membrane. In this case, it is possible to identify ulcerative defects, their number, area and exact location.
- Functional state of the colon.
The study is contraindicated if there is a suspicion of perforation of the intestinal wall.
Colonoscopy
This is the most informative method for diagnosing diseases of the large intestine.
Special equipment is used for the study. The examination is carried out with the introduction, through the anus into the cavity of the large intestine, of a flexible endoscope and a miniature high-resolution camera. The image with a high degree of magnification is displayed on the monitor.
Colonoscopy:
- detects the presence of ulcers;
- determines their quantity and location;
- assesses the affected area.
During the procedure, a tissue sample is always taken for biopsy. This is necessary to assess the degree and quality of changes in the morphology of the cellular composition of tissues taken from the surface of the ulcerative defect, and to exclude malignancy.
According to individual indications, the procedure is performed under anesthesia.
Sigmoidoscopy
This is an endoscopic method for examining the lower parts of the colon. During the procedure, both soft plastic and hard metal sigmoidoscopes are used.
During the examination, the doctor:
- assesses the condition of the wall of the anus, rectum and sigmoid colon;
- detects the presence of defects (ulcers, cracks, wounds, hemorrhoids);
- determines the presence of possible neoplasms (polyps, tumors);
- excludes possible invaginations of the mucous membrane and internal prolapse of the intestine.
In addition to a visual examination, tissue is taken from pathological lesions for a biopsy. In addition, therapeutic manipulations are often performed during the examination - cauterization of a bleeding vessel, removal of a polyp, etc.
Differential diagnosis of colon ulcer
Many diseases of the colon have symptoms and diagnostic signs similar to ulcers.
Additional research methods are required for differential diagnosis.
Crohn's disease
Chronic inflammatory bowel disease. The pathological process covers not only the colon, but also the distal parts of the small intestine.
An endoscopic examination reveals features characteristic of Crohn's disease: linear ulcers alternating with foci of bulging mucosa - “cobblestone syndrome”.
Nonspecific ulcerative colitis
The disease is autoimmune hereditary in nature. The patient's medical history usually contains information about cases of illness in the family.
Clinically, exacerbation of UC is accompanied by signs of inflammation and intoxication:
- increased temperature;
- general malaise;
- joint pain.
In a blood test for nonspecific ulcerative colitis, signs of autoimmune inflammation are detected - a high content of class G immunoglobulins.
Ischemic colitis
The pathology develops due to impaired blood supply to the large intestine, which occurs for various reasons. As a result, due to lack of oxygen, foci of necrosis (death of tissue areas) form on the surface of the mucous membrane and in the muscular layer of the intestinal wall.
The disease is characterized by mature age of patients - over 40 years. Most often, ischemic colitis occurs as a complication of chronic diseases of the cardiovascular system - atherosclerosis, heart defects, aortic aneurysm, ischemic heart disease, etc.
Characterized by an acute onset and severe pain. The condition, according to vital indications, requires emergency medical care, including comprehensive hospital-based measures.
Shigellosis
This is a group of intestinal infectious diseases that have a common pathogen - bacteria of the genus Shigella. The parasite affects all parts of the large intestine.
The main symptoms are diarrhea mixed with blood and mucus, signs of intoxication. For differential diagnosis, bacteriological examination of stool is performed.
Amoebiasis
A group of parasitic diseases caused by unicellular protozoa. Intestinal and extraintestinal forms are observed. Damage to the liver and skin is typical.
An accurate diagnosis can be made by examining stool: microscopic examination of biological material reveals parasites. A serological blood test determines antibodies to the pathogen.
Neoplasms
Many symptoms of colon ulcers are similar to those of benign or malignant tumors.
X-ray and endoscopic methods help to identify neoplasms and differentiate them from ulcers. To determine the nature of the tumor, a biopsy is performed with histological examination of the materials.
Irritable bowel syndrome
This is a functional disorder that is characterized by frequent episodes of abdominal pain, with changes in the nature and frequency of stool. Among the reasons, psychosocial factors occupy an important place - stress, depression, neuroses.
When performing colonoscopy and sigmoidoscopy, structural changes in the mucous membrane, in most cases, are not detected.
Haemorrhoids
The disease is varicose veins of the hemorrhoidal plexus of the rectum. Pathological changes develop outside and/or inside the rectum, as well as the anal canal.
The disease is accompanied by acute pain, bleeding during and after defecation. A differential diagnosis will be made by digital examination of the rectum and endoscopic methods. With hemorrhoids, characteristic nodes are identified that have a purplish-bluish color.
Laparoscopic gastric surgery
The stomach is rightfully considered the central link of the human digestive system. Diseases that primarily affect the stomach subsequently inevitably lead to disruption of the functioning of the entire gastrointestinal tract. Modern gastroenterology today has a sufficient arsenal of means and methods for treating most diseases of the stomach. However, there are a number of situations where therapeutic methods are no longer effective. In addition, a whole group of diseases, based on the development of tumors in the stomach, obviously does not initially involve therapeutic methods of treatment. In these cases, the question naturally arises of whether the patient should undergo surgical treatment.
Even in the recent past, gastric operations were widely performed using traditional laparotomy (open) access. Currently, an increasing number of clinics, both abroad and in Russia, are switching to the use of laparoscopic technologies in gastric surgery. Fundamentally, the scope of surgical intervention does not change when using laparoscopic technologies. At the same time, due to the minimal trauma of laparoscopic interventions (including the absence of a surgical wound), fast and smooth postoperative rehabilitation of patients is ensured, there are no cosmetic defects on the anterior abdominal wall and the risk of wound complications, including the development of postoperative hernias.
In the Department of Abdominal Surgery of the Federal State Budgetary Institution “Clinical Hospital No. 1 (Volyn)”, UDP of the Russian Federation, a number of laparoscopic surgical interventions are used in the surgical treatment of patients with gastric pathology:
— laparoscopic fundoplication – gastroesophageal reflux disease (GERD) / hiatal hernia (HH);
— laparoscopic longitudinal sleeve gastrectomy – morbid obesity/metabolic syndrome;
— laparoscopic distal subtotal gastrectomy with regional lymphadenectomy D2+ — stomach cancer;
— laparoscopic gastrectomy with regional lymphadenectomy D2+ — stomach cancer;
— laparoscopic partial gastrectomy – neuroendocrine tumors/stromal tumors;
— laparoscopic suturing of perforated ulcers of the stomach and duodenum — peptic ulcer of the stomach/duodenum, complicated by perforation.
Principles of treatment of colon ulcers
Treatment tactics depend on the cause, severity of the disease and the presence of complications.
Treatment for colon ulcers includes:
- surgical methods;
- medications;
- a carefully selected diet.
Traditional medicine can be used with the permission of the attending physician and under his supervision.
Surgical treatment
Indications for surgical treatment of colon ulcers are the ineffectiveness of conservative methods and the development of complications - bleeding, perforation, intussusception and others.
Types of operations
The type and technique of surgical intervention depend on the size and location of the ulcer, as well as the presence of complications.
To eliminate an ulcer:
- Endoscopic operations - a flexible optical part of the equipment and microsurgical manipulators are inserted through the anus.
- Laparoscopic minimally invasive interventions - instruments are inserted through small punctures in the anterior abdominal wall.
- Open, extensive interventions - classic operations with dissection of the anterior wall of the abdominal cavity.
In the absence of complications, surgeons tend to perform minimally invasive operations. They are the least traumatic, have minimal blood loss and allow you to heal colon ulcers in a short time.
Recovery period
After the operation, the patient spends in the hospital from 2 to 10 days (depending on the volume and method of intervention). The surgeon prescribes painkillers.
Meals should be fractional and sparing. Patients are advised to get out of bed as early as possible and move more (walk on a straight, level surface). Physical activity is prohibited for 1.5-2 months.
Possible consequences and prognosis for life
If the operation is performed in a timely and correct manner, the patient complies with all the doctor’s instructions, the postoperative prognosis is usually favorable.
However, there is always a risk of developing:
- bleeding;
- wound infection;
- cicatricial narrowing of the intestinal lumen;
- adhesive disease.
The risk of these complications increases if the patient has previously undergone intestinal surgery.
Drug therapy
The goals of drug therapy are to relieve inflammation, restore motility and normalize intestinal microflora. Main groups of drugs:
- antibacterial drugs selected taking into account the sensitivity of pathogenic flora;
- probiotics – “Maxilak”, “Normobakt”, etc.;
- antidiarrheal drugs - Smecta, Loperamide, Imodium;
- antispasmodics - “No-shpa”, “Papaverine”, “Platifillin”;
- laxatives - Bisacodyl, Duphalac, Glycelax.
Medications are prescribed in the form of tablets for oral administration and rectal suppositories. To speed up the healing process, Sucralfate is used in the form of therapeutic enemas.
Diet
Along with medications, proper nutrition plays an important role in the treatment of colon ulcers. Fried, spicy and smoked foods, coarse fiber, coffee, carbonated and alcoholic drinks are excluded from the diet.
Products are served boiled or baked and eaten warm. Slimy soups and porridges, jelly, and vegetable purees are useful.
Treatment with folk remedies
Treatment of colon ulcers with tablets and suppositories can be combined with folk recipes. This can only be done under the supervision of the attending physician.
You can treat the symptoms of colon ulcers at home with herbal remedies:
- Wound healing - yarrow, plantain, tansy.
- Eliminates pain and inflammation - chamomile, oregano, galangal, etc.
- Laxatives - dill, flaxseed, senna, buckthorn.
Herbal decoctions and infusions are taken orally or administered as enemas.
Introduction
Over the past 15 years, drug therapy has been a priority in the treatment of gastric ulcer (GPU) and duodenal ulcer (DU). The development and improvement of surgical interventions for peptic ulcers and peptic ulcers has sharply slowed down due to the successful complex use of H2 receptor antagonists, proton pump inhibitors (PPIs), and anti-Helicobacter therapy. This revolutionary step in therapy has led to the fact that the need for elective surgical treatment of uncomplicated peptic ulcer disease has been minimized. As a rule, gastric resection is used for complicated course of ulcerative gastric ulcer and peptic ulcer. At the same time, drug treatment did not completely eliminate relapses of gastric ulcers and ulcers and recurrent bleeding [2, 4]. In this regard, the number of complications of peptic ulcer disease, such as perforation, bleeding, stenosis, and penetration, does not decrease. All these complications of peptic ulcer disease require surgical treatment.
A serious argument in limiting the indications for planned surgical treatment of peptic ulcer disease was the high traumatic nature of open surgical access, a significant number of immediate and late postoperative complications, long treatment periods and disability after open gastrectomy (ORG). All these shortcomings were eliminated as the technique of laparoscopic gastrectomy (LGR) improved.
The emergence of laparoscopic technologies in surgery made it possible to develop and introduce into surgical practice LRZ for peptic ulcer disease.
In February 1992, P. Goh and C. Kum [7] performed successful laparoscopic resection of ⅔ of the stomach according to Billroth II. It would seem that a new direction in the surgery of peptic ulcers and peptic ulcers will be widely promoted by surgeons. Indeed, in Russia the first laparoscopic gastric resections took place in 1994-1995. completed O.E. Lutsevich [3], V.P. Sazhin [5] and V.N. Egiev [1]. By 2000, the experience of performing LRZ for peptic ulcer disease had grown and crossed the line of 70 operations. However, from 2000 to the present, the total number of LRGs performed for gastric and duodenal ulcers in Russia is unknown.
It should be recognized that laparoscopic operations on the stomach have not become widespread to this day. However, this trend is also typical for other abdominal diseases. According to A.V. Fedorov and V.E. Olovyanny (2011), “...no more than 30% of general surgeons use the laparoscopic method. Among all interventions on the abdominal organs, laparoscopic operations account for about 20%” [6].
In 2010-2012 Surgical websites on the Internet demonstrate successful options for performing laparoscopic gastrectomy for gastric ulcers and peptic ulcers, but in the medical literature there are no results of generalized and systematic studies on this problem.
The purpose of the study is to conduct a comparative assessment of the results of open and laparoscopic gastric resections for complicated gastric and duodenal ulcers.
Material and methods
In the period from 1994 to 2012, we performed laparoscopic gastrectomy in 84 patients with a complicated course of gastric ulcer and peptic ulcer. All surgical interventions were performed using the Billroth-II technique modified by Dubourg. The results of LRZ were compared with the results of treatment of 99 patients who underwent LR. The structure of diseases during laparoscopic and open gastrectomy is presented in Table. 1
.
In both groups, patients with existing ulcerative gastroduodenal bleeding (UGDB) predominated.
In case of PU, LRZ was performed in 58.3% of patients, in case of DU - 41.7% of patients. Approximately the same ratios were in the group of patients who underwent ORG - 56.6 and 43.4%, respectively. Both groups are comparable in age (the average age of patients was 58.3±3.7 years) and gender (men predominated 77.6±1.1%). They had various concomitant diseases. Gastric ulcers were localized mainly in the body of the stomach, on the lesser curvature (75.4%). The size of the ulcers ranged from 0.8 to 3 cm (average 1.9±0.5 cm). The depth of the ulcers ranged from 0.6 to 1.1 cm (average 0.9±0.3 cm). Duodenal ulcers were localized mainly on the posterior wall (62.7%). The size of duodenal ulcers averaged 1.1±0.5 cm, depth - 0.7±0.2 cm.
Between 1994 and 1999, 61 gastric resections were performed laparoscopically. This period was characterized by active surgical tactics for complicated peptic ulcer disease. In 1994, the number of gastric resections in the total structure of gastric resections was 3%, in 1999 - 30%.
Since 2001, due to a change in the treatment tactics of patients with ulcerative gastrointestinal tract with an emphasis on drug therapy for perforated ulcers with a transition to laparoscopic suturing and subsequent drug treatment, the number of patients requiring gastric resection, including laparoscopic, has decreased significantly. In the period from 2001 to 2012, LRZ was performed in 23 patients, i.e. on average 2 operations per year.
The objectives of the study included a comparative assessment of the immediate, immediate and long-term results of traditional and laparoscopic operations, the acid-producing function of the stomach at different times after operations performed by traditional and laparoscopic methods, and their functional effectiveness.
Results and discussion
One of the important results of assessing the technical performance of LRG is the duration of the operation. The duration of LRG at the initial stages of mastering the technique was 6 hours 15 minutes. The initial period of performing LRZ was characterized by the use of a large number of clips to clamp the transected vessels. Sometimes, when mobilizing the stomach, the number of clips reached 50 pieces. With the improvement of instruments and surgical techniques, the duration of LRZ was reduced to 3.5 hours. The use of devices such as Harmonic and LigaSure played a special role in reducing the operation time. Thanks to higher technical availability, this indicator can be reduced to 2-3 hours (on average to 2.2 ± 0.22 hours).
In the immediate postoperative period, only one patient after LRG was diagnosed with a complication—a hematoma of the anterior abdominal wall.
After POR, postoperative complications occurred in 28 (28.3%) patients, after LSR - in 1 (1.2%) patient. The structure of postoperative complications was dominated by suppuration of postoperative wounds. The very technology of performing LRZ made it possible to exclude from the structure of complications the most typical for traditional surgery, such as suppuration of the surgical wound.
The low-traumatic technique of LVG and early activation of patients made it possible to avoid the development of acute adhesive intestinal obstruction and pulmonary embolism.
After ORG, the mortality rate was 4.0%; after LRG, there were no deaths (Table 2)
.
The volume of LRG and ORG in peptic ulcer disease in all patients amounted to ⅔ of the organ.
The LRG technique for PU and DU was fundamentally similar. Individual characteristics of the operation depended on topographic-anatomical changes associated with the localization of the ulcer and ulcerative infiltrate. In 4 (4.8%) cases with LPG, certain technical difficulties were encountered due to the low location of the ulcer and its penetration into the pancreas. They were overcome by careful step-by-step laparoscopic tissue preparation. No intraoperative complications were identified in these patients.
A comparative assessment of the long-term results of LRZ and ORZ according to the Visick criteria did not reveal any significant differences (after ORZ, excellent and good results were observed in 71.9% of patients, after LRZ - in 84.8% of patients). The best indicator for LVG can be explained by the standard technique of forming gastroenteroanastomoses using staplers, low traumatic operation and low blood loss. LRZh and ORZh differ in the technology of execution, the degree of technical complexity, methods of treatment and removal of the ulcerative defect. From this point of view, assessing results only according to Visick criteria is insufficient. The scoring system proposed by Johnston (1980) and modified by Yu.I. seems more objective. Kiselev and P.M. Postolov (1981). This system made it possible to differentiate the severity of each postoperative syndrome (Table 3)
.
Depending on the frequency and severity of a particular symptom, the results of the operation were assigned a certain number of points. The sum of points obtained based on the results of different operations was compared, keeping in mind that the optimal results are obtained by the operation that received the lowest number of points according to this rating system.
The PCM assessment allowed us to obtain 1193.6 points, and the LRG score - 732.2 points. The lower number of points for LGC is explained primarily by the absence of deaths and relapses of the disease. Hypoglycemic and dumping syndrome, as well as diarrhea occurred after LRG in a milder form. As a result, in terms of long-term functional results, they turned out to be 1.6-1.8 times more effective than ORZh.
To study the acid-producing function of the stomach, we used the aspiration-titration method and the method of computer intragastric pH-metry. Among 183 patients who underwent LGC and ORG, hyperacidity was detected in 1 (1.2%) and 4 (4.0%) patients, respectively. The result of the Hollander test in one of these patients, who had undergone acute gastrointestinal tract infection, was positive, and in the postoperative period he was diagnosed with a peptic ulcer of the gastroenteroanastomosis. In all other observations, regardless of the method of surgical intervention, a state of achlorhydria or a state of hypoacidity close to it was established.
Thus, LRZ for peptic ulcer disease, thanks to constantly improving instruments and equipment, is much more effective than similar open operations. Postoperative complications after LRG developed in 1.2% of cases versus 28.1% after ORG. More advanced technology for performing LRZ for peptic ulcers made it possible to avoid mortality and improve long-term functional results by 1.6-1.8 times.
Prevention of occurrence, relapses and complications of colon ulcers
Prevention of ulcers includes prevention of the primary process and the development of relapses.
The main measures are:
- proper balanced nutrition;
- dosed physical activity, avoiding overloads;
- normalization of intestinal microflora.
Patients with chronic inflammatory bowel diseases or who have undergone surgery should be regularly monitored by a doctor and undergo courses of anti-relapse treatment.
Oncological processes and colon ulcers
Chronic recurrent ulcers of the large intestine are included in the group of precancerous conditions along with polyps. Cancer can develop 7-10 years after signs of a colon ulcer appear.
The incidence of malignancy ranges from 6 to 12%. The five-year survival rate in such patients is no more than 20%. For primary cancer this figure is 50%.
Alertness and risk groups
Categories of patients at risk for developing cancer complications have been identified.
These include:
- patients whose symptoms of colon ulcers appeared in childhood or adolescence;
- people with a hereditary predisposition;
- patients with concomitant diseases (in particular, diabetes mellitus);
- men who regularly smoke tobacco products.
Provoking factors may be other bad habits (overeating, physical inactivity, alcoholism), unbalanced diet, contact with carcinogens in connection with professional activities.