Intestinal metaplasia - what is it?
Intestinal metaplasia is a disease in which tissue from the stomach lining is replaced by intestinal cells. The disease was first described by Professor Kupfer more than 100 years ago.
Elderly people are most often affected. According to statistics, 80% of those infected are diagnosed with chronic gastritis, as well as duodenal ulcer.
In a healthy state, the tissues that cover the walls of the stomach are constantly renewed. When damaged, cell division increases, which leads to increased migration and restoration of cellular renewal. In patients diagnosed with chronic gastritis, this process is disrupted, resulting in the inability of the gastric glands to perform their functions, which leads to metaplasia.
Features for different parts of the stomach: antrum, pyloric region
Metaplastic changes can occur in any part of the stomach, occupying only part of the mucosa or the entire thickness. The lesions are located in the membrane of the body, fundus or pyloric region, less often in the antrum.
The stomach is a rather complex organ
Important! Pathological changes in the gastric mucosa are considered a precancerous condition, so the disease is classified as dangerous. Studies conducted by many scientists have confirmed the presence of metaplasia in 94% of patients suffering from stomach cancer.
Observations over the past two decades have confirmed that tissue changes in intestinal metaplasia and intestinal type gastric cancer (Lauren classification) are completely identical.
Doctors believe that intestinal cancer occurs under the influence of external carcinogenic factors (substances that cause cancer). Most often occurs in the body of the stomach. Studies have shown that the disease develops in complex epidemiological areas.
METAPLASIA
METAPLASIA
(
metaplasia
; Greek metaplasso to transform, transform) is a persistent transformation of one type of tissue into another, morphologically and functionally different from the original. Metaplasia is an adaptive process, with the help of which the tissue survives in changed conditions of existence due to structural restructuring, in contrast to histological accommodation, when the cells do not change tissue-specific structural properties. The term was first proposed in 1884 by R. Virchow. The doctrine of Metaplasia was intensively developed in the first half of the 20th century. in the works of Hansemann (DP Hansemann), Ribbert (M. WH Ribbert), Krompecher (E. Krompecher), H. G. Khlopin, G. E. Koritsky and others.
There are direct and indirect Metaplasia. Direct Metaplasia is characterized by a change in the nature of the tissue without the proliferation of its cells. A typical example of direct M. is the transformation of connective tissue into bone without the participation of osteogenic elements. In indirect, or neoplastic, M. proliferation of cells with their reproduction and differentiation is observed. Sometimes the newly formed tissue can reach a higher degree of development than was typical of the original tissue, for example, the formation of liver tissue with M. of the bile duct epithelium, the formation of pancreatic islets with M. of the pancreatic duct epithelium. Then the process is designated as prosoplastic M. In some cases, cell differentiation turns out to be lower than in the original tissue, which is called regressive M., for example. with the development of multilayered squamous epithelium in place of the cylindrical ciliated epithelium of the mucous membrane of the respiratory tract.
The cause leading to M. is most often chronic, inflammation, dishormonal changes, tumor process, vitamin A deficiency.
Depending on the location of the changes, M. is isolated from epithelium, connective tissue with its transformation into bone and cartilaginous tissue, and the so-called. myeloid M. with the transformation of lymphoid cells into cells of the myelopoietic series. Epithelial M. is more common; an example of a cut is the transformation of the epithelium of the sebaceous and salivary glands in conditions of hron, inflammation into stratified squamous keratinizing epithelium, the epithelium of the mammary and sweat glands with dishormonal changes - into pale epithelium of the apocrine type. Known as intestinal M., or enterolization of the gastric mucosa, for example, with gastritis, as well as epidermoid M. of the epithelium of the gallbladder, bile ducts and pancreatic ducts, which occurs during chronic inflammation. The transitional epithelium of the urinary tract during hron, inflammation can be subjected to M. in both squamous multilayer epithelium and glandular prismatic epithelium. In the mesodermal epithelium, the possibility of transformation of mesothelium into fibroblasts is noted.
According to a number of authors, M. can be carried out over a wide range and the transformation of the epithelium into connective tissue is possible (see Mesenchyplasty). Other authors limit M. to the histogenetic type, denying the possibility of transformation of epithelium, for example, of the endodermal type, into epidermal. Some authors deny the possibility of M., explaining the appearance of epithelium alien to a given place by embryonic dystopia, heteroplasia, prosoplasia, pluripotency of cambial elements and various directions of their differentiation. The most widely accepted point of view is one that recognizes the possibility of extensive transformations of epithelial tissue, but denies the possibility of transformation of epithelium into connective tissue.
Wedge, M.’s value depends on the etiology and localization of the patol, the process. In the mucous membrane of the cervical canal and in the endometrium, areas of stratified squamous epithelium are found in cases of uterine prolapse, pyometra, tuberculosis, etc. More often, true M. is observed, carried out with the help of reserve cells. According to some authors, the epithelium of the cervix with dishormonal disorders can be subjected to M. in the glandular prismatic; epithelium of the endometrial glands - into the epithelium of the glands of the cervix and fallopian tubes; the epithelium of the glands of the cervix - into the epithelium of the endometrial glands and fallopian tubes. The epithelium of the epididymis during chronic inflammation can become similar to the transitional epithelium of the urinary tract. M. epithelium of the oral mucosa and cervix into stratified squamous keratinizing epithelium is a precancerous disease (see); an unfavorable prognostic sign is the appearance of foci of squamous cell M. in layers of transitional cell carcinoma.
Bibliography
Golovin D.I. About epithelial metaplasia, M., 1958, bibliogr.; Malignant tumors, ed. N.N. Petrova, vol. 1, part 1, p. 83, L., 1947; Korlatsan V.V. On the question of the histogenesis of stomach cancer and the role of intestinal metaplasia in this process, Arch. pathol., t. 39, v. 3, p. 39, 1977; Paykova L.V. Superficial gastric cancer, Vopr, onkol., t. 18, no. 4, p. 31, 1972, bibliogr.; Popova E.A. Variability of the uterine and vaginal epithelium in vitamin A deficiency, Arch. pathol., t. 20, v. 9, p. 59, 1958; Raikhlin H. T., Romanenko A. M. and Opperman A. New morphological methods in oncology (using the example of tumors from the transitional epithelium), M., 1977; Samsonov V. A. Tumors of the bladder, M., 1978; Sarkisov D. S. Regeneration and its clinical significance, M., 1970; Ackerman LV a. Regato JA Cancer, diagnosis, treatment and prognosis, St. Louis, 1962; Christoffersen J.a. Moller JE Adenomatoid tumors of the urinary bladder, Scand. J. Urol. Nephrol., v. 6, p. 295, 1972; Handbuch der normalen und pathologischen Physiologie, hrsg. v. A. Bethe ua, Bd 14, T. 2, S. 1211, B., 1927; Kawachi T. ao Studies of intestinal metaplasie in the gastric mucosa, J. nat. Cancer Inst., v. 53, p. 19, 1974; O'Flunn JD a. Mullaney J. Vesical leukoplakia progressing to carcinoma, Brit. J. Urol., v. 46, p. 31, 1974; Schridde H. Die Ortsfremden Epithel-gewebe des Menschen, Jena, 1909; Widran J., Sanches Ra Gruhn J. Squamous metaplasie of the bladder, J. Urol. (Baltimore), v. 112, p. 479, 1974.
D. I. Golovin.
Types of metaplasia of the gastric mucosa
There are two types of disease:
- complete (small intestine, mature);
- incomplete (colon, immature).
Mature metaplasia is characterized by the presence of cells that are found only in the small intestine: border cells, sulfamucines, goblet enterocytes. But the main sign confirming this type of disease is Paneth cells. The tissues of the stomach resemble the small intestine not only in structure, but also in functional properties.
With immature metaplasia, there is a disturbance in the maturation and development of the gastric glands: the upper layers are practically no different from the lower ones. The epithelium mainly consists of cells of the large intestine.
The complete type of intestinal metaplasia is more common, and in most cases is detected in patients with chronic gastritis. It is believed that this is a transitional stage to colonic metaplasia.
Important! According to statistics, an incomplete form of stomach cancer is detected in 94% of cases. Therefore, the disease is considered a precancerous condition, which, if not treated promptly, can lead to death.
According to the type of prevalence of the lesion, they are distinguished:
- weak – localization on 5% of the mucosal surface;
- moderate – up to 20%;
- pronounced – more than 20%.
Doctors distinguish intestinal metaplasia according to the type of pathology:
- pyloric - the tubular glands in the body of the stomach are replaced by mucous. They are called "Sterck's pyloric glands." Found, as a rule, with atrophic gastritis;
- ciliated - characterized by the appearance in the digestive tract of ciliated cells, which are absent in a healthy person. Doctors believe that their formation is associated with the development of metaplasia. In addition, the pathology occurs with a malignant tumor - adenocarcinoma. However, this type of disease does not always lead to stomach cancer;
- pancreatic – quite rare. It is classified by the appearance of fine-grained texture cells in the mucosal tissues.
Focal and diffuse forms
Additionally, focal and diffuse forms of development of the anomaly are distinguished in pyloric metaplasia.
With the focal type, replacement of some tubular glands occurs against the background of inflammation and damage to the cellular renewal of the gastrointestinal tract. Diffuse pathology is characterized by damage to the gastric mucosa without disruption of the structure and death of cells.
Classification of metaplasia
There are 2 types of gastric metaplasia:
- Full mature or small intestine. Has a benign course.
- Incomplete immature or colonic. More dangerous than the previous form, it often develops into a malignant tumor.
But there may also be a mixed form, when cells of the small and large intestines are found in the epithelium of the stomach at the same time.
Based on the size of the area occupied by altered cells, metaplasia is divided into several forms:
- weak - 5% of the area of the gastric mucosa is occupied by altered cells;
- moderate – 20% of the surface is affected;
- severe - more than 20% of the mucosal surface is affected.
According to the degree of atrophy of the glands, they are distinguished:
- minor degree - type A;
- intermediate degree - type B;
- full degree - type C.
Also, according to the nature of distribution, the following are distinguished:
- Focal metaplasia - characterized by partial, small-area cell replacement, most often found in the pyloric and antral zone, against the background of inflammatory changes in the mucous membrane and when cell renewal processes are disrupted.
- Diffuse form - intestinal metaplasia is found in the pyloric and antrum, can move further, occupy a large area and involve the mucous membrane of the fundus.
Complete small intestinal metaplasia
The mature form of metaplasia is characterized by the fact that all the cells characteristic of the small intestine appear in the structure of the gastric mucosa. But the most reliable sign is the appearance of Paneth cells with characteristic apical granulation. They are found in the pits together with borderless enterocytes.
The gastric mucosa resembles the small intestine in structure and functional and morphological properties.
The complete, mature form of metaplasia is found much more often than the incomplete one. It is considered a transitional form to the immature colonic type. But they can be combined within the same gland or found in different glands.
This type of disease often accompanies chronic gastritis.
Incomplete colonic metaplasia
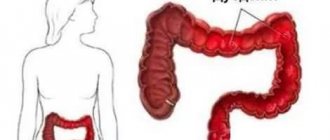
In the case of colonic metaplasia, the altered areas are characterized by the presence of cells that normally line the inner surface of the large intestine. With this form, Paneth cells are not found in the stomach. With incomplete colonic metaplasia, cell maturation and differentiation are impaired; this is a sign of a precancerous condition.
With this form of metaplasia, the gastric mucosa, in structure and functional properties, acquires features characteristic of the large intestine.
This type of metaplasia is considered more dangerous and less predictable in predicting the outcome of the disease.
In benign diseases, signs of colonic metaplasia are found in 11% of patients, in stomach cancer - in 94%.
Causes
The main reasons for the development of the disease include:
- inflammation of the gastric mucosa caused by various factors;
- gastrointestinal irritation;
- chronic esophagitis - inflammation of the tissues of the esophagus;
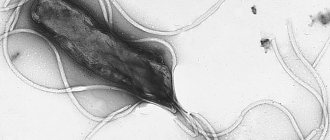
- long-term gastritis - especially with increased stomach acidity. In most cases, the development of metaplasia is associated with the bacterium Helicobacter pylori. The microorganism affects the immune system and adapts to its changes, causing damage to the gastric epithelium of varying severity;
- frequent stressful situations;
- chronic reflux - esophagitis - exposure to irritating factors on the mucous membrane of the esophageal walls for more than six months. Inflammation occurs when gastric juice leaks or leaks into the esophagus;
- hormonal disorders.
Symptoms of the disease
Intestinal metaplasia itself does not manifest itself. All symptoms relate to ailments that preceded its development. Doctors identify the main signs of the disease:
- nausea;
- aching pain in the epigastric region;
- loss of appetite.
The epigastric region is the part of the abdomen in the upper, middle area just below the ribs
With increased acidity of the stomach, heartburn and “hunger” pains are observed, which intensify at night. If the disease is accompanied by reflux of gastric contents into the esophagus, vomiting and a feeling of bitterness in the mouth may occur.
Symptoms
There are no characteristic signs indicating metaplasia. Complaints are made in accordance with the causal factors that caused the disease.
With gastritis with high acidity, the patient feels:
- frequent burning sensation in the epigastrium;
- hunger pains;
- hunger during night sleep.
The main complaints with reflux disease with frequent reflux of bile into the stomach:
- for diffuse pain;
- bitterness in the mouth;
- vomiting
Diagnostics reveals an imbalance in the motility of the antral zone of the stomach and reverse peristalsis.
Histology will indicate focal metaplasia of the antrum of the organ.
If the process is provoked by a peptic ulcer:
- intense, local pain;
- hunger pains that subside after eating.
Regular periods of spring-autumn exacerbations.
Endoscopy shows changes in the mucous membrane characteristic of an ulcer - erosions, scars.
Helibacteriosis has symptoms similar to chronic gastritis. The diagnosis is confirmed by examination of biomaterial taken from the mucosa, in which waste products of the microorganism are detected, and a respiratory test, that is, examination of the air exhaled by the patient, and stool analysis.
General symptoms common to all patients with metaplasia:
- belching with a bitter or sour taste;
- the appearance of periodic pain in the upper abdomen;
- frequent attacks of nausea, sometimes vomiting;
- decreased appetite.
Diagnosis of the problem
The diagnostic standard is considered to be histological examination, which reveals the form of the disease. During the procedure, small pieces of tissue taken from the human body are examined. The method of collecting cells or epithelium is called a biopsy. This is a mandatory way to confirm the diagnosis if the formation of malignant tumors is suspected.
To determine the extent of damage, an additional examination of the gastrointestinal tract is carried out using endoscopic equipment with cell staining. Suspected pathological tissues are tinted with a special paint - methylene blue, which is absolutely safe for human health. Damaged cells acquire a special color and become visible under a microscope.
A combination of methods allows you to diagnose the disease more accurately. In addition, the degree of identification of the bacterium that causes chronic gastritis is increasing, and the need to identify it in intestinal metaplasia in order to prevent a precancerous condition is increasing.
Intestinal metaplasia - treatment
To properly begin treatment, the doctor must get a complete picture of how widespread intestinal metaplasia is in the digestive system. To do this, endoscopy is performed. Once the diagnosis is confirmed, the doctor will recommend various treatments to reduce the progression of intestinal metaplasia.
If an H. pylori infection is suspected, your doctor will prescribe a course of antibiotics, including:
- amoxicillin;
- metronidazole;
- clarithromycin;
- tetracycline.
Antibiotic treatment usually lasts about 2 weeks.
The doctor may also recommend medications that reduce acidity.
Certain dietary changes can prevent intestinal metaplasia. These usually involve eating a diet rich in natural foods such as vegetables, fruits, nuts and whole grains. These foods contain nutrients and antioxidants.
People who have gastrointestinal disorders such as GERD should avoid fried, fatty or spicy foods. Salty foods may also be a culprit in intestinal metaplasia. Reducing salt intake helps prevent intestinal metaplasia.
Features of treatment
Therapy depends entirely on the degree of damage to the mucosa. If metaplasia is detected, the patient is registered with a gastroenterologist.
Drug therapy
Treatment with medications is primarily aimed at:
- elimination of gastroesophageal reflux disease - a disease in which the acidic contents of the stomach are regularly thrown into the esophagus. Under the influence of acid, damage to the mucous membrane occurs;
- suppression of gastric secretion;
- destruction of the bacteria H. pylori;
- prevention of benign neoplasms.
The treatment regimen is developed only by the attending physician, taking into account the results of the examinations. Therapy begins with the appointment:
- Proton pump inhibitors are modern medications that reduce the acidity of gastric juice. These include: rabeprozole, omeprozole, pantoprazole;
- antacids (Maalox, phosphalugel) - agents that neutralize hydrochloric acid;
- H2 – histamine blockers (cimetidine, ranitidine) – antisecretory drugs;
- gastroprotectors - in case of increased acidity of the stomach, they prevent the destruction of the mucous membrane.
Pregnancy and childhood are restrictions for taking certain medications.
To enhance the effect, first-line antibacterial agents (amoxicillin, clarithromycin) are additionally prescribed. The course of treatment is 7–10 days. In case of ineffectiveness of therapy, as well as low sensitivity of the infection to these drugs, second-line antibiotics (tetracycline, metronidazole) are prescribed.
The use of inhibitors increases the pH of the stomach, reduces the viscosity of gastric mucus, and prevents the destructive effect of antibacterial drugs. It is necessary to take into account that at the same time you should take medications that strengthen the immune system and prevent the development of dysbacteriosis.
Surgical intervention
Surgery is recommended if there is no positive effect on conservative treatment. In order to minimize the area of intervention in the body and the degree of injury, operations are performed using special endoscopic equipment. This type of surgery is called minimally invasive surgery. It is characterized by a limited depth of damage to the mucous membrane. If necessary, the damaged area is completely removed. As a result of the procedure, the risk of carcinogenic formations is significantly reduced.
Diet
Treatment will not be complete without proper nutrition. Patients are recommended:
- exclude dairy products from the menu, as well as those that irritate the gastric mucosa (fried, spicy, salty);
- do not drink alcohol, coffee, carbonated drinks;
- meals should be fractional, at least 5–6 rubles/day;
- last meal – 2–3 hours before bedtime;
- The diet must include fresh vegetables and fruits.
Nutritionists advise introducing a variety of cereals into your diet. It is recommended to eat food only warm.
Too hot food irritates the gastric mucosa, while cold food takes a long time to digest and provokes the release of hydrochloric acid.
Photo gallery: foods you can eat
You can eat steamed meat. It retains many beneficial substances for the body, which are so necessary during illness.
Fresh and steamed vegetables will not harm the stomach and will be an excellent addition to the diet
The absorbent properties of rice porridge are successfully used to effectively remove toxins and waste.
The use of folk remedies
Traditional medicine offers no less effective methods of combating the disease. Decoctions and infusions of medicinal herbs and herbs reduce signs of inflammation and relieve pain.
- Herbal mixture of chamomile, calendula, yarrow and marshmallow root. Take 1 tsp. each herb, mix and steam 0.5 liters of boiling water. Leave in a thermal container for about an hour. Filter and take 3-4 times a day for 30 minutes. before meals, 20 ml.
- Pour boiling water over flax seeds (1 tbsp) and boil for 5 minutes. Leave for 1-2 hours, take 30 ml before each meal.
- St. John's wort. Grind 15 gr. dried herbs, steam 200–250 ml of boiling water. Leave to infuse in a thermos for 12 hours, preferably overnight. Filter the mixture and bring the volume to 250 ml. Take 30 minutes before. before meals, 50 ml of infusion. The course of treatment is 14 days, then take a week break.
Photo gallery: popular folk remedies in the treatment of gastric metaplasia
St. John's wort has astringent properties, prevents the appearance of malignant neoplasms
Chamomile, yarrow, calendula, calamus root have an anti-inflammatory and wound-healing effect
A decoction of flax seeds protects the mucous membrane from the harmful effects of gastric juice
Complications
In a healthy person, epithelial cells are constantly renewed. Under the influence of harmful factors (alcohol, long-term use of medications, poor diet), the mucous membrane gradually changes. If treatment is not started in time, the inflammatory process becomes chronic.
Gastric metaplasia develops against the background of concomitant diseases and successive changes.
Chronic gastritis caused by the Helicobacter bacteria leads to complications such as:
- glandular atrophy – pathological changes in the mucous membrane;
- dysplasia – a violation of the epithelium and its functional properties;
- Neoplasia of the gastric mucosa is the first sign of cancer.
Some scientists have scientifically proven that chronic gastritis, the bacterium Helicobacter pylori, intestinal metaplasia, atrophy and stomach cancer are links in one chain in which a microorganism becomes a provocateur. As a result of infection, chronic inflammation is formed in the mucous membrane, and tissue degeneration occurs, provoking the development of intestinal-type stomach cancer.
Against the background of atrophic chronic gastritis, in which the irreversible disappearance of the gastric glands occurs with their replacement by altered tissues, gastrointestinal cancer develops in 75% of cases.
In addition to the bacterium H. pylori, other types of microorganisms appear that produce carcinogenic and mutagenic substances that accelerate the risk of tumors.
In addition, atrophic hCG leads to impaired secretion of internal factor and a decrease in the production of hydrochloric acid. As a result, the normal absorption of vitamin B12 is disrupted, which leads to anemia and neurological disorders.
The gastric mucosa is replaced by metaplastic epithelium, which leads to irreversible processes and the development of cancer
Kinds
Classification by type can be defined as small intestinal (complete) and large intestinal (incomplete). Both conditions are quite dangerous, caused by various reasons with mandatory medical correction.
- Small intestinal complete metaplasia is most often caused by the presence of chronic gastritis and leads to the formation of foci of changes. A characteristic sign of complete metaplasia is the detection of Paneth nuclei (cells) in the epithelium of the gastric mucosa. The altered tissues not only form the walls of the small intestine, but also begin to function in the same way.
- Colonic metaplasia is even more dangerous. In this pathology, the epithelium of the stomach consists almost entirely of cells of the large intestine. The normal process of formation of the gastric glands, as well as its digestive function, is disrupted. This condition is a precancerous threat, because in more than 94% of patients with stomach tumors the process began this way.