Chronic gastritis: symptoms and treatment in adults at home
Chronic gastritis is a disease of the stomach that lasts for quite a long period of time and its characteristic features are disruption, changes in the composition and inflammation of the gastric mucosa; with untreated gastritis, ordinary epithelial glands lose their ability to regenerate and begin to be replaced by connective tissue.
In the process of obvious disorders, progress is made in changing the gastric structure, accompanied by serious functional disorders, which is expressed in the secretory secretions of hydrochloric acid and pepsin. Chronic gastritis can be briefly described as inflammation of the gastric mucosa. This disease affects about 70% of the world's population, and chronic gastritis itself has many subtypes that require treatment when exacerbations occur.
Causes
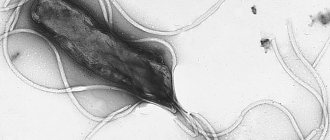
Modern medicine identifies the bacterium Helicobacter pylori, which is located in the human stomach and duodenum, as the cause of chronic gastritis.
These bacteria affect more than 70-80% of the adult population. Every year the number of diseases among children increases. In developing countries, infection rates are higher than in developed countries. Most often, the disease occurs in residents of Asia and Latin America. The risk of its development increases every year and does not depend on gender.
The causes that contribute to the occurrence of chronic gastritis are divided into exogenous (external) and endogenous (internal).
Exogenous causes:
- consumption of alcoholic beverages;
- prolonged use of medications;
- smoking on an empty stomach (nicotine tones blood vessels and spasms capillaries, which worsens blood circulation in the stomach tissues);
- violation of the diet (snacks on the go, insufficient chewing), bad habits (eating spicy, fatty, sour foods), eating very cold and hot foods;
- hazardous production (under conditions of the presence of harmful substances in the air and high dust levels).
Endogenous causes include:
- chronic inflammation of the lungs and upper respiratory tract;
- pulmonary failure;
- endocrine diseases (diabetes mellitus, hypothyroidism, disorder of corticosteroid synthesis);
- metabolic disorders (gout, enzyme deficiency, insulin resistance);
- immunity disorder, which is characterized by the production of antibodies to body tissues;
- liver cirrhosis, chronic pancreatitis, hepatitis, which contribute to the development of pathology of the gastric glands, change the environment and damage the mucous membrane.
Classification
Chronic gastritis is divided into:
| Form of bronchitis | Description |
| Autoimmune form (type A) | A rather rare pathology, characterized by the death of a large number of mucosal cells in all parts of the stomach. The reason for the development is a disruption of the immune system. The body's protective cells perceive normal healthy mucosal cells as foreign. They begin to produce specific antibodies that actively fight against them. |
| Bacterial form (type B) | It develops against the background of damage to the stomach wall by the Helicobacter bacterium. Infection often becomes the cause of the development of erosive gastritis. |
| Chemical form (type C) | Causes: reflux of bile into the stomach, long-term use of NSAIDs, operations performed on the gastrointestinal tract, congenital or acquired pyloric insufficiency (valve between the yolk and duodenum). Characterized by an increase in histamine levels. As a result, the alkalinity of bile increases. By acting on the walls of the stomach, bile provokes inflammation, the formation of erosions, and bleeding. |
| Mixed form of gastritis (type A and B) | Acidity can be low or high. |
There are two forms of chronic gastritis: superficial and atrophic. In superficial cases, the upper layers of the mucous membrane are affected. In 98% of cases, this type is not accompanied by pathological changes in the glands. The atrophic form is more severe. It is characterized by serious consequences - the wall of the stomach becomes thinner, the number of glands decreases. All these processes lead to secretory insufficiency.
Gastritis polypous
Description
Polypous gastritis is a special form of chronic gastritis, characterized by atrophy and dysregenerative hyperplasia of the gastric mucosa, achlorhydria. Etiology, pathogenesis It is often a complication of chronic gastritis with secretory insufficiency, combined with rigid gastritis. Gastric polyps consist of a connective tissue base of the integumentary (papilloma) or glandular (adenoma) epithelium. They have a stalk or a wide base. The shape of the polyps resembles a berry or cauliflower. Their consistency may vary. Polyps are most often located on the anterior and posterior walls of the antrum of the stomach. Symptoms There is no typical clinical picture. There is a tendency of patients to bleed. In 1/3 of patients, the transition of polyposis to a cancerous tumor is observed. Prognosis Due to frequent malignancy, the prognosis of polypous gastritis is very serious. When a pedunculated polyp is localized in the prepyloric region, it may prolapse into the duodenum, resulting in the development of pyloric stenosis. With cancerous degeneration or prolapse of a polyp into the duodenum, bleeding is observed.
First signs
General signs of chronic gastritis in adults are identified. These include:
- aching, paroxysmal pain in the stomach after eating;
- hunger pains at night;
- diarrhea followed by constipation;
- gas formation, stomach rumbling;
- decreased appetite leads to weight loss;
- pale skin, sleep disturbance;
- belching and heartburn (a sign of low acidity);
- lump in the throat, pain in the esophagus and burning;
- heaviness, feeling of fullness in the stomach;
- nausea and vomiting after each meal or medication (a sign of low acidity).
Sometimes a person only feels occasional pain and bouts of nausea. This means gastritis occurs secretly.
Rigid gastritis
Description
Rigid gastritis is a special form of chronic gastritis, characterized by pronounced deep inflammatory scarring changes predominantly in the antrum of the stomach, its deformation and narrowing. Symptoms Pain in the epigastric region, dyspepsia, increased secretion of gastric juice, rarely achlorhydria. Diagnosis X-ray examination reveals a tube-shaped narrowing of the pylorus, which presents differential diagnostic difficulties with the tumor. The diagnosis is confirmed by gastrofibroscopy with targeted biopsy and dynamic observation of the patient.
Symptoms of chronic gastritis
For a long time (especially at the beginning of the disease), chronic gastritis in adults occurs without visible symptoms. In the development of the disease, as a rule, there are periods of remission and exacerbation.
During periods of exacerbation, short-term attacks of pain, discomfort in the upper abdomen, a feeling of heaviness, nausea after eating, and heartburn may appear, which indicates a dysfunction of the natural “valves” of the stomach and the reflux of acidic stomach contents into the esophagus. Signs of impaired digestion of food in the intestines may also appear: episodes of constipation or diarrhea, bloating (flatulence), increased rumbling.
Symptoms of chronic atrophic gastritis:
- decreased appetite;
- unpleasant taste in the mouth;
- nausea after eating;
- constipation or diarrhea;
- bloating, rumbling in the stomach, flatulence;
- belching with an unpleasant putrid odor;
- feeling of fullness, heaviness in the stomach after eating;
- dull pain immediately after eating or after 15-20 minutes;
- anemia, brittle and dry hair, split nails.
Often the disturbances in the digestive process described above lead to weight loss, severe weakness, drowsiness, and irritability of a person. As already mentioned, chronic gastritis occurs with periodic exacerbations and remissions. During remission, the symptoms of the disease practically disappear, but reappear during the period of exacerbation of the disease.
Exacerbation of chronic gastritis can be seasonal (for example, in spring and autumn), and can also be provoked by poor diet, smoking, alcohol, and the use of certain medications.
Characteristic features of gastritis remission
At the stage of remission, the state of the body largely coincides with the early period of the disease - superficial gastritis. Modern medicine diagnoses chronic gastritis using a gastroscopy procedure. Main features:
- The mucous surface of the stomach is in most cases slightly thickened. With complete remission, the membrane returns to its normal state.
- The integumentary pitted epithelial tissue has dystrophic changes that are almost imperceptible. During the process of restoration of the body, the highly columnar epithelium is deformed into cubic epithelium and becomes flattened.
- The nuclei become hyperchromic and increase in size.
- Positive material indicating hypersecretion of the gastric lining is found above the cell nuclei in the cytoplasm.
- A mucous layer forms on the surface of the epithelial tissue.
- Suppression of secretion is rarely diagnosed.
- In the apical part of the cells, a mucoid appears in the form of a narrow, small strip. The number of RNAs increases significantly.
- A pronounced lymphoplasmacytic infiltration is noticed in the lamina of the human gastric mucosa.
- The remission stage is characterized by the intactness of the antrum and glands in the human body.
Intact antrum
During the period of remission of the disease in the patient’s body, there is a complete or partial absence of signs of gastritis. Often manifests itself in people with chronic exacerbation of the disease. At this stage, the patient expects the possible completion of strict but effective measures for the treatment of chronic gastritis. Temporary prophylaxis and constant monitoring by the attending physician for possible exacerbation of the disease should not be ruled out.
Chronic gastritis in the remission stage takes different periods of time, from a week to decades - if a person follows the norms prescribed by the treating doctor. Then the course of remission depends entirely on the complex of treatment prescribed by the doctor.
Many aspects of recovery depend directly on the effectiveness of the recommendations and the abandonment of the patient’s aggravating bad habits. In the last stage of gastritis, it is necessary to minimize the obvious manifestation of symptoms and signs. A person takes a break from treatment for many years.
Low or high acidity
With increased acidity of the stomach, excessive production of hydrochloric acid is observed. It not only digests food, but also irritates the mucous membrane. High acidity is especially insidious during periods of famine. The acid kills beneficial bacteria and causes ulcers to form on the surface of the stomach.
A person experiences the following symptoms:
- Belching sour;
- Unpleasant sour taste in the mouth;
- Severe heartburn;
- Burning in the stomach and esophagus;
- Hunger pain that occurs on an empty stomach and goes away immediately after eating.
Gastritis with high acidity can be recognized by other signs:
- Arrhythmia;
- Irritability, depression;
- Drowsiness, fatigue;
- Decreased blood pressure;
- Heartache.
With low acidity, little hydrochloric acid is formed in the stomach. Its quantity is not enough for complete digestion of food. This leads to the fact that the food lies in a lump at the bottom of the stomach and begins to rot.
As a result, the patient experiences the following symptoms:
- Diarrhea;
- Bad breath, rotten taste;
- Nausea present all day;
- Bloating, flatulence, colic;
- Feeling of hardness in the stomach area;
- Aching pain in the pit of the stomach immediately after eating;
- Unpleasant belching of air immediately after eating;
- Poor appetite, requires a small portion of food to feel full;
- In advanced cases, vomiting of undigested pieces of food.
The listed symptoms are concomitant signs of the presence of chronic gastritis. But they can also indicate a number of other diseases, so you should not make a diagnosis yourself, relying only on sensations.
Making the correct diagnosis
Inspection, palpation, percussion, and auscultation do not play a decisive role in recognizing the disease.
An important place is occupied by determining the state of acid-forming functions. For these purposes, it is recommended to stop taking medications that affect the level of acidity in the stomach 1–2 days before the examination.
Laboratory and instrumental studies may include:
- Study of the secretory function of the stomach.
- Stool analysis: possible presence of hidden blood, as well as undigested food debris with reduced secretory activity of the stomach.
- Manometry: with reflux gastritis, an increase in pressure in the duodenum to 200-240 mm water column is detected. (normally - 80-130 mm water column).
- A general blood and urine test will help detect signs of an inflammatory process in the body during exacerbation of chronic gastritis (in remission, tests will be normal), hyperchromic anemia in chronic autoimmune gastritis.
- Identification of the microbe Helicobacter pylori. The “gold standard” is a histological examination of biopsy specimens with their staining according to certain schemes and subsequent microscopic examination. A biological method is also used (seeding a microorganism on a nutrient medium).
- FGDS and taking biopsies for histological examination. If it is impossible to perform FGDS, an X-ray examination of the stomach with barium contrast can be performed, but this is less informative.
Differential diagnosis is carried out with peptic ulcer of the stomach and duodenum, diaphragmatic hernia, esophagitis, and tumors.
What to do if you suspect a disease
Blood chemistry
In autoimmune chronic gastritis, hyperbilirubinemia and hyper-γ-globulinemia are observed.
Immunological studies
With autoimmune chronic gastritis, there is a decrease in IgA and IgG, an increase in the level of B-lymphocytes and T-helpers by more than 6 times, and the appearance of autoantibodies to parietal cells and gastromucoprotein.
Fibroesophagogastroduodenoscopy
In autoimmune chronic gastritis, the gastric mucosa is atrophic, the antrum is without pathology.
X-ray
In autoimmune chronic gastritis, the folding of the gastric mucosa is not pronounced.
Treatment of chronic gastritis
The choice of treatment regimen for chronic gastritis depends on the form of the disease. Treatment is usually carried out at home, but if complications develop, patients require hospitalization.
- Patients with low acidity of gastric juice are prescribed drugs that stimulate secretory activity.
- For patients with increased gastric secretion, antisecretory, antacid drugs (to relieve heartburn), and prokinetics are indicated.
In the acute period of gastritis, abstain from eating until the gastric mucosa heals independently and the symptoms disappear; Drinking (tea, Borjomi) is allowed. After this, normal food intake is gradually resumed: first, following a gentle diet, then, when the gastric mucosa is completely restored, increasing the amount of food consumed.
The basic principles of treating gastritis are: reducing or eliminating the consumption of alcohol and caffeine, as well as spicy foods; quitting smoking and using medications that reduce dyspepsia and heartburn. Prescription of vitamin preparations may be required. In some cases, the use of medications is indicated.
Nutritional therapy is of great importance in the treatment of gastritis. During the period of exacerbation of gastritis, meals should be fractional, 5-6 times a day. The diet is prescribed by the doctor depending on the acidity of the gastric juice. Physiotherapy and mineral water treatment are prescribed.
Gastritis hemorrhagic
Description
Hemorrhagic gastritis is a special form of chronic gastritis, characterized by a tendency to gastric bleeding, predominantly inflammatory and erosive changes in the gastric mucosa, preserved or high gastric secretion. Etiology In some cases, bleeding is associated with increased vascular permeability of the stomach and mild trauma to its mucosa, taking non-steroidal anti-inflammatory drugs, and alcohol. Symptoms Symptoms of gastric bleeding - vomiting “coffee grounds” or tarry stools, general phenomena caused by a decrease in circulating blood volume - fainting, tachycardia, a sharp decrease in blood pressure up to collapse. Diagnosis: Endoscopic examination, which reveals swelling, hyperemia and mild contact bleeding of the gastric mucosa, multiple flat defects (erosions) and petechiae.
Drug treatment
The following groups of drugs are used in the treatment of chronic gastritis in adults:
- Enzyme preparations are necessary to normalize digestive processes. These include Mezim, Creon, Pancreatin.
- Antacids are prescribed to relieve heartburn because they have the ability to bind hydrochloric acid and reduce the activity of gastric enzymes. These include Almagel, Phosphalugel, Gaviscon.
- Antibacterial drugs are prescribed when a H. pylori infection is detected in a patient’s stomach. To destroy them, various groups of antibiotics can be used, which are selected only by a doctor.
- Drugs that reduce the secretion of hydrochloric acid. These include H2-histamine receptor blockers (Famotidine, Ranitidine) and proton pump inhibitors (Nexium, Omez).
- Drugs that stimulate gastric secretion (plantain juice, Limontar) are prescribed for chronic gastritis with decreased secretory function of the stomach.
- Normalization of peristalsis and elimination of spasms is achieved with the help of antispasmodic drugs (No-shpa, papaverine) and drugs that regulate motility (Trimedat).
- Vitamins are included in therapy in cases where, as a result of a long-term inflammatory process in the stomach, vitamin deficiency and anemia have developed. Patients are usually prescribed iron supplements (Sorbifer-durules, Ferlatum), vitamin B12 and folic acid.
- Drugs that have a gastroprotective effect help protect the gastric mucosa from the aggressive effects of hydrochloric acid and gastric juice. They have an astringent and enveloping effect. Drugs in this group include De-nol, Vikalin. The drug Venter, in addition to the above effects, has an antacid and antiulcer effect.
The use of folk remedies for the treatment of chronic gastritis is acceptable, but before using them you should consult your doctor.
Diagnostics
The diagnosis of chronic gastritis is quite possible to make based on existing clinical symptoms, however, to confirm its autoimmune nature, it is necessary to conduct the following studies:
- CBC: decrease in the number of red blood cells, hemoglobin, platelets, leukocytes, increase in the numbers of the color index.
- Blood biochemistry: hyperbilirubinemia, hyper-γ-globulinemia.
- Immunological examination: decrease in IgA and IgG, increase in the level of B-lymphocytes and T-helper cells by more than 6 times, the appearance of autoantibodies to parietal cells and gastromucoprotein.
- Gastric secretion: decreased acid and pepsin formation, achlorhydria.
- FGDS: the gastric mucosa is atrophic, the antrum is without pathology.
- R-scopy of the stomach: folding of the mucous membrane is not pronounced.
- Histomorphological study: replacement of specialized glands with pseudopyloric and intestinal epithelium.
Diet for chronic gastritis
When treating chronic gastritis, patients are prescribed a gentle diet, the preparation of which takes into account the acidity of gastric juice. The main goal of the diet for chronic gastritis is to minimize thermal, mechanical, and chemical irritation of the stomach, reduce inflammation and stimulate the healing processes of the mucous membrane.
- During exacerbations of chronic gastritis, it is necessary to avoid eating too hot or too cold food; it is recommended to steam or boil food, serve it in a liquid or puree state. The diet can include lean meat and fish, eggs, cereals, and rosehip decoction. It is necessary to exclude the consumption of coffee, carbonated drinks, chocolate, raw vegetables and fruits, flour products, fermented milk products, fatty, fried foods, and spices.
- During the period of remission of chronic gastritis, split meals are recommended for patients with high acidity. Products that can stimulate the secretion of hydrochloric acid, such as meat broths, alcoholic beverages, tea, and strong coffee, are excluded from the diet. Also excluded are spicy, smoked, fatty, fried foods, canned food, and some vegetables (onions, radishes, white cabbage, sorrel).
During remission, patients with chronic gastritis with low acidity are not recommended to consume foods that linger in the stomach for a long time (for example, flour products, rice). You should also refrain from eating hot, spicy, smoked foods that irritate the gastric mucosa.
Acute gastritis
Description
Acute gastritis is an acute inflammation of the gastric mucosa. — Simple gastritis — Catarrhal gastritis — Corrosive gastritis — Phlegmonous gastritis Etiology, pathogenesis Polyetiological disease caused by chemical, mechanical, thermal and bacterial causes. Pathogenesis boils down to dystrophic-necrobiotic damage to the surface epithelium and glandular apparatus of the gastric mucosa and the development of inflammatory changes in it. The inflammatory process can be limited to the superficial epithelium of the mucous membrane or spread to the entire thickness of the mucous membrane, interstitial tissue, and even the muscular layer of the gastric wall. Symptoms usually appear 4–8 hours after exposure to the etiological factor. Characterized by a feeling of heaviness and fullness in the epigastric region, nausea, weakness, dizziness, vomiting, diarrhea. The skin and visible mucous membranes are pale, the tongue is coated with a grayish-white coating, drooling or, conversely, severe dry mouth. Palpation reveals pain in the eligastric region. Diagnosis It is necessary to exclude salmonellosis and other intestinal infections. Bacteriological and serological studies are of decisive importance. Treatment Begins with cleansing the stomach and intestines, and in case of infectious etiology of gastritis, prescribing antibacterial drugs (enteroseptol 0.25–0.5 g 3 times a day, chloramphenicol 2 g/day, etc.) and absorbent substances (activated carbon, kaolin, etc.). For acute allergic gastritis, antihistamines are indicated. For severe pain, use anticholinergic drugs and antispasmodics. For dehydration, parenteral administration of an isotonic solution of sodium chloride and 5% glucose solution. In case of chlorpenic syndrome, hypertonic sodium chloride solution is administered intravenously. For acute vascular insufficiency, cordiamine, caffeine, mesaton, norepinephrine are indicated. For the first 1–2 days it is recommended to abstain from eating, but you are allowed to drink small portions of strong tea, Borjomi; On the 2nd–3rd day, low-fat broth, slimy soup, semolina and pureed rice porridge, and jelly are allowed. Then the patient is transferred to diet No. 1, and after 6–8 days - to normal nutrition. Classification There are simple, catarrhal, corrosive and phlegmonous acute gastritis. Simple gastritis Etiology, pathogenesis It occurs most often. The causes of exogenous gastritis are errors in nutrition, food toxic infections, the irritating effect of certain drugs (salicylates, butadione, bromides, digitalis, antibiotics, sulfonamides), food allergies (to strawberries, mushrooms, etc.), etc. Endogenous acute gastritis occurs when acute infections, metabolic disorders and massive breakdown of proteins (in case of burns, etc.). Acute gastric irritation can develop with severe radiation injuries. Catarrhal gastritis Pathogenesis There is infiltration of superficial, sometimes dystrophic, necrobiotically altered epithelium by leukocytes, as well as signs of inflammatory hyperemia. The prognosis is favorable if treatment is started in a timely manner. If the effect of harmful factors is repeated, then acute gastritis usually becomes chronic. Corrosive gastritis Etiology Develops due to the ingestion of strong acids, alkalis, heavy metal salts, and concentrated ethyl alcohol into the stomach. Symptoms Pain in the mouth, behind the sternum and in the epigastric region, often unbearable, repeated painful vomiting; in the vomit - blood, mucus, and sometimes tissue fragments. On the lips, mucous membranes of the mouth, pharynx and larynx - traces of a chemical burn - swelling, hyperemia, ulceration (grayish-white spots appear from sulfuric and hydrochloric acid, yellow and greenish-yellow scabs from nitric acid, brownish-red from chromic acid, bright white ones from carbolic acid, reminiscent of a lime coating , from vinegar - superficial whitish-gray burns). When the larynx is damaged, hoarseness and wheezing appear. In severe cases, collapse develops. The abdomen is usually swollen, painful on palpation in the epigastric region; Sometimes signs of peritoneal irritation are detected. Acute perforation occurs in 10–15% of patients in the first hours after poisoning (less often later). Treatment Begins with gastric lavage with plenty of cold water through a probe lubricated with vegetable oil (contraindications to the insertion of a probe are collapse and destruction of the esophagus). Before washing, especially in case of pain, narcotic analgesics (morphine hydrochloride, promedol), fentanyl with droperidol are indicated. In case of collapse, in addition, caffeine, cordiamine, mesaton, norepinephrine (s.c. or i.v. with blood replacement fluids, glucose, isotonic sodium chloride solution), as well as strophanthin. During the first days - fasting, parenteral administration of isotonic sodium chloride solution, 5% glucose solution. If it is impossible to feed by mouth over the next few days, parenteral administration of plasma and protein hydrolysates. In case of gastric perforation or laryngeal edema, urgent surgical treatment is required. To prevent narrowing of the esophagus, bougienage is performed during the healing period; if the latter is ineffective, surgical treatment of stenosis is performed. Prognosis Depends on the severity of inflammatory-destructive changes and therapeutic tactics in the first hours and days of the disease. The life-threatening period of illness lasts 2-3 days, death can occur from shock or peritonitis. The outcome of corrosive gastritis can be scar changes, especially in the pyloric and cardiac parts of the stomach. Phlegmonous gastritis Etiology, pathogenesis It is rare, characterized by phlegmonous inflammation of the stomach wall with diffuse or limited distribution of pus mainly in the submucosal layer; usually recognized during surgery. Usually accompanied by the development of perigastritis and often peritonitis. Occurs more often primarily; is caused by streptococci, often in combination with Escherichia coli, less often staphylococcus, pneumococcus, Proteus, etc. Sometimes it develops as a complication of an ulcer or disintegrating stomach cancer, damage to the gastric mucosa due to abdominal trauma. The secondary form develops during general infections (sepsis, typhoid fever, etc.). Symptoms Characterized by acute development with chills, fever, severe weakness, pain in the upper abdomen, nausea and vomiting. The tongue is dry, the stomach is swollen. The general condition is deteriorating sharply. Patients refuse to eat and drink, quickly become exhausted, and facial features change (the face of Hippocrates). In the epigastric region there is pain on palpation. In the blood there is high neutrophilic leukocytosis with toxic granularity, increased ESR, changes in protein fractions and other signs of inflammation. Prognosis: Unfavorable in many cases. Complications are possible (purulent mediastinitis, pleurisy, subphrenic abscess, thrombophlebitis of large abdominal vessels, liver abscess, etc.). Treatment is carried out mainly in surgical hospitals. Broad-spectrum antibiotics are administered parenterally in large doses. If conservative therapy is ineffective, surgical treatment is performed.
Consequences of gastritis
Gastritis (with the exception of phlegmonous gastritis) does not belong to the group of dangerous diseases. However, gastritis gives rise to dangerous complications:
- Stomach bleeding
- Peptic ulcer of the stomach and duodenum,
- Stomach cancer.
The effect of gastritis on the body as a whole is explained by a disorder of the digestive process. Patients with gastritis begin to “fear food”, lose weight, some vomit most of the food they eat, or suffer from heartburn after eating. Against the background of gastritis, vitamin deficiency and anemia often develop.