What is gastrectomy?
Resection (removal) of the stomach (code according to the international classification of diseases K91.1) is necessary when conservative treatment methods become powerless. It is prescribed to patients diagnosed with cancer, peptic ulcers, polyps and other diseases of the gastrointestinal tract. Gastric surgery is performed in several ways:
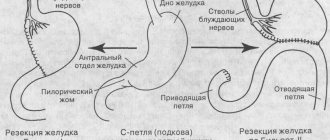
- Partial resection of the lower part of the stomach, when the preserved part is connected to the duodenum.
- Partial resection of the upper part of the stomach, when the upper area, which is involved in the pathological process, is excised, and then a subsequent connection of the esophagus is made to the lower part of the organ.
- Sleeve (longitudinal) gastroplasty. This type of operation is used in the treatment of obesity, when most of the stomach is removed while preserving the natural connections of the duodenum and esophagus.
- Complete gastrectomy, when the entire organ is removed and then a connection is made between the duodenum and the final part of the esophagus.
Cost of gastric resection in Israel
In Israel, a personalized approach to the treatment of each patient is used. This means that all diagnostic and treatment regimens are selected individually depending on the disease, the patient’s well-being, the course of the disease, etc.
That is why the cost of Billroth operations is calculated individually for each person. In order for the medical center staff to freely calculate the cost of the operation specifically in your case, fill out the feedback form, attaching all the tests you have.
Find out the cost of treatment
In order to receive detailed information about Billroth operations in Israel, fill out an application or contact us at the specified phone numbers, and in order to receive an individual estimate and clarify the prices for gastrectomy in Israel, fill out the “Calculation of the cost of treatment” form. Within 24 hours, managers are guaranteed to provide you with all the necessary information.
Indications for surgery
Absolute indicators for resection are malignant tumors of the stomach, when surgery gives the patient a chance to prolong life. Doctors prescribe surgical intervention when ulcers do not heal for a long time, the acidity of gastric juice is reduced, or severe scar changes occur that give a pronounced clinical picture.
Stomach cancer
All organs of the human body are made up of cells that grow and divide when new cells are needed. But sometimes this process is disrupted and begins to proceed differently: cells begin to divide when the body does not need it, and old cells do not die. Additional cells accumulate, forming tissue that doctors call a tumor or neoplasm. They can be benign or malignant (cancerous).
Stomach cancer begins in the inner cells, but over time invades the deeper layers. In this case, the tumor can grow into neighboring organs: the esophagus, intestines, pancreas, liver. The causes of malignant neoplasms of the stomach are divided into several types:
- poor nutrition, especially associated with the abuse of fried, canned, fatty and spicy foods;
- smoking and alcohol;
- chronic diseases of the gastrointestinal tract: ulcers, gastritis;
- hereditary predisposition;
- hormonal activity.
Severe stomach ulcer
An ulcer is a defect in the gastric mucosa. Peptic ulcer disease is characterized by periodic exacerbations, especially in the spring and autumn. The main reason for the development of the disease is frequent stress, which strains the nervous system, which causes muscle spasms in the gastrointestinal tract. As a result of this process, a malfunction in the nutrition of the stomach occurs, and gastric juice has a detrimental effect on the mucous membrane. Other factors leading to the development of peptic ulcers:
- disrupted diet;
- chronic gastritis;
- genetic predisposition;
- long-term medication use.
With a chronic gastric ulcer, the formation of ulcerative defects occurs on the mucous membrane of the organ. Resection of these pathologies is performed when complications of the disease develop, when there is no effect from conservative therapy, bleeding occurs, and stenosis develops. This is the most traumatic type of surgery for stomach ulcers, but also the most effective.
- Caprese salad recipe with photos step by step
- Charlotte with sour cream - step-by-step recipes for baking a lush dessert at home with photos
- DIY curtain tiebacks
Laparoscopic resection for obesity
Laparoscopic surgery is an endoscopic method of gastric surgery, which is performed through punctures in the abdominal cavity with a special instrument without a wide incision. This resection is carried out with the least trauma for the patient, and the cosmetic postoperative result is much better. The indication for laparoscopic gastrectomy is the extreme stage of obesity, when neither medication nor a strict diet helps the patient.
With obesity, a metabolic disorder occurs, and when the process of losing weight can no longer be controlled, doctors have to remove part of the stomach, after which the patient gets rid of the problem, loses weight and gradually returns to everyday life. But the biggest advantage of laparoscopy is the restoration of normal metabolism, reducing the risk of atherosclerosis and coronary heart disease. Watch the video to see how laparoscopic gastrectomy is performed:
Stomach operations
Gastrostomy (gastric fistula)
- Upper-median laparotomy
(see page 125). During the inspection, the surgeon evaluates the detected changes and selects a place to place a gastrostomy. - Fistula application
. With four napkins inserted into the corners of the surgical wound, the surgeon isolates the free abdominal cavity. By this time, the sister should prepare a gastrostomy tube 30-40 cm long from soft rubber, which can be made from a thick gastric tube that has been repeatedly boiled. The surgeon places the tube along the longitudinal axis of the stomach. Above the tube, 7-8 interrupted sutures made of silk No. 4 are placed on the wall of the stomach so that a tunnel 4 cm long is formed from this wall; two or three sutures at the end of the tube are not tied. After this, a rigid clamp is applied to the second end of the tube, and the nurse delivers a scalpel to open the lumen of the stomach. First, the tip of an electric suction is inserted into the resulting hole and the contents are evacuated, and then the proximal end of the tube is inserted and fixed to the gastric wall with an interrupted catgut suture No. 6 or No. 8, stitching the rubber and the stomach. Previously placed sutures are tied. At this stage, several additional stitches may be necessary: the nurse should have needle holders loaded with silk on hand. To check the patency of the rubber tube, remove the clamp from its outer end and insert a funnel through which a small amount of isotonic sodium chloride solution is injected into the stomach, after which the clamp is applied to the tube again. - Bringing the tube out.
The gastrostomy tube is usually brought out in the area of the left rectus abdominis muscle. To do this, use the same techniques as when removing drainage through a counter-aperture (see p. 126), only the skin is not pierced with a scalpel, but pulled out in the form of a cone with a Kocher clamp and excised with a scalpel in the form of a circle.
After this, the barrier napkins are removed, and the tube is passed through the thickness of the abdominal wall using a forceps. From the inside, the anterior wall of the stomach is sutured to the peritoneum with interrupted silk sutures. After making sure that the sutures are tight, the surgeon sutures the wound of the anterior abdominal wall in layers. On the operating table, the gastrostomy tube should be closed to prevent leakage of gastric contents.
Gastrotomy (opening the lumen of the stomach)
- Upper-median laparotomy.
- Opening the lumen of the stomach. The surgeon grabs the anterior wall of the stomach with a damp gauze pad and guides it into the wound. Isolates the stomach with napkins. Two holders made of silk No. 4 are placed on the front wall of the stomach. The threads for the holders need to be 35-40 cm long. A clamp is applied to both threads of each holder. The nurse hands the surgeon a scalpel and prepares No. 2 catgut threads on an intestinal needle for puncturing and ligating the vessels of the submucosal layer. The surgeon incises the wall of the stomach in the longitudinal direction, punctures the vessels of the submucosal layer and ligates them; The ends of the catgut threads are cut off with scissors. Using the same scalpel, the surgeon opens the mucous membrane for 1.5-2 cm and throws the scalpel into the pelvis. By this time, the nurse should prepare the tip of the electric suction, which is inserted into the resulting hole. After suctioning out the stomach contents, the mucous membrane is cut along the required length with scissors. Narrow abdominal speculum may be needed to examine the stomach. The further course of the operation depends on the nature of the detected pathology. The operation is completed by applying sutures to the stomach: first, the nurse applies a long catgut thread No. 4 on a round needle to apply a continuous suture, then, after cutting off the ends of the catgut thread, short (20-25 cm) silk No. 4 threads, also on a round needle for application second row of interrupted sutures.
- Layer-by-layer suturing of the anterior abdominal wall.
Suturing of a perforated ulcer of the stomach and duodenum
- Upper-median laparotomy.
- Abdominal toilet.
Immediately after opening the abdominal cavity, the contents are evacuated with tampons, or better yet, with the help of an electric suction. After this, the nurse gives the surgeon four large tampons, which he inserts deep into the abdominal cavity around the stomach and duodenum. - Suturing the perforation hole.
The sister feeds silk No. 4 threads 25-30 cm long on a round needle; the surgeon applies 4-5 interrupted sutures in the transverse direction, sometimes placing a strand of the greater omentum under the suture line. - Repeated toilet of the abdominal cavity
. Tampons placed before suturing are removed. The surgeon carefully drains the abdominal cavity with tuffers. - Layer-by-layer suturing of the anterior abdominal wall.
Gastroenteroanastomosis
- Upper-median laparotomy.
- Preparation of a loop of small intestine for anastomosis.
a) If the small intestine is located behind the colon, this stage of the operation begins with opening the gastrocolic ligament, which requires 6-8 hemostatic clamps, scissors, and No. 4 catgut ligatures. Assistants stretch the transverse colon, and the surgeon dissects its mesentery in an avascular area with scissors. He then selects a site for anastomosis on the small intestine and marks it with silk and catgut sutures (No. 4), passing them into the mesentery of the small intestine using a pointed clamp. Both threads with clamps placed on them and a loop of the small intestine are passed through an opening in the mesentery of the transverse colon and the latter is immersed in the abdominal cavity. The surgeon positions the intestinal loop so that the silk thread (beginning) is above the anastomosis site, and the catgut thread (end) is below the anastomosis site. b) When the small intestine is located in front of the colon, the place on the small intestine is marked in the same way and the loop is brought over the colon and omentum to the anterior wall of the stomach (or to the posterior wall - after opening the gastrocolic ligament). - Anastomosis
. The first point of this stage of the operation is the application of stay sutures that limit the size of the future anastomosis. For the holders, the sister places two silk No. 4 threads 40 cm long on an intestinal needle. Then interrupted silk (No. 2) sutures are placed on the posterior lip of the anastomosis without opening the lumen of the stomach and intestines; silk threads 25-30 cm long are fed on an intestinal needle. After applying this series of sutures, the nurse gives the surgeon scissors to cut off all threads except the outermost ones, and napkins to isolate the surgical field before opening the lumen of the gastrointestinal tract. At the moment of opening the lumen, the nurse should immediately turn on the electric suction or prepare several lush tuffers. Usually, to prevent the entry of contents, the wall of the stomach at the site of the anastomosis is pressed with a soft curved gastric sponge. The intestinal lumen is also closed with one or two soft intestinal clamps. Parallel to the line of sutures, the surgeon uses a scalpel to incise the seromuscular membrane of the stomach and intestines. After this, he can either immediately open the lumen of both organs with scissors and perform hemostasis, capturing the bleeding vessels with clamps supplied by the nurse, or ligate the vessels first, before opening the lumen. In this case, the surgeon pricks the vessels visible in the submucosal layer with a round thin needle loaded with catgut or silk (at the surgeon’s discretion) thin (No. 0, No. 1) threads. Threads are pricked and tied on both sides of the intended dissection of the mucous membrane of both organs; after opening the lumen, there is no bleeding, and the surgeon proceeds in a calm atmosphere to the next stage of the operation. This stage consists of applying an internal row of sutures - a continuous catgut suture (No. 2) first on the posterior and then on the anterior wall of the anastomosis. After cutting off the ends of the hemostatic sutures with scissors, the operating nurse provides the surgeon with a catgut thread 40-50 cm long on a round intestinal needle, and the assistant with anatomical tweezers and several gauze balls for periodic drying of the suture line. At the same time, the nurse must ensure that the small balls, as they are used up, are dropped one by one into the pelvis and do not remain in the area of the surgical field. After tying a continuous thread and cutting off its ends with scissors, gloves are processed, napkins and tools are changed. The surgeon begins to apply a second row of sutures on the anterior wall of the anastomosis, for which the nurse applies silk threads No. 2, 16-20 cm long, on a round intestinal needle. After this, the clamps are removed from the stomach and intestines. - Application of enteroenteroanastomosis.
Typically, gastroenteroanastomosis is supplemented by the imposition of an anastomosis between the afferent and efferent loops of the intestine in a side-to-side manner (see “Enteroenteroanastomosis”). - Abdominal toilet
. Isolating napkins are removed from the abdominal cavity, the cavity is dried, and the nurse counts the presence of instruments and material. - Layer-by-layer suturing of the wound of the anterior abdominal wall.
Gastric resection according to Billroth II (Hofmeister-Finsterer modification)
- Upper-median laparotomy.
- Revision of the abdominal organs
. The nurse gives the surgeon a napkin to fix the stomach, and the assistant a liver speculum. Large tampons are inserted through mirrors inserted into the abdominal cavity, the mirrors are moved from under the tampons on top of them and the surrounding tissues are removed with mirrors. - Mobilization of the stomach
. The purpose of this stage of the operation is to achieve mobility of the stomach by intersecting the tissues that fix it. To separate the stomach along the greater curvature, the nurse gives the surgeon a pointed clamp, which makes two holes in the gastrocolic ligament. Then she gives the surgeon and the assistant one hemostatic clamp each to apply a ligament to the resulting strand (Fig. 89, a). In this sequence, everyone works until the nurse has 2-4 clamps left, about which she must promptly warn the surgeon. After this, ligation begins. To ligate the part of the gastrocolic ligament remaining in the body, the nurse applies strong catgut (No. 6) threads. As a rule, the ligament contains fatty tissue and the threads slide when tied, so they must be of sufficient length (25-30 cm). Silk ligatures No. 6 are applied to the part that leaves with the stomach. After releasing all the clamps, mobilization continues in the same order as before. When manipulating near the duodenum and pancreas, the surgeon may need 2-4 thin Mosquito-type clamps and strong, thin No. 2 silk ligatures 20-25 cm long. After releasing the entire greater curvature, the nurse gives a long curved clamp, with which the surgeon makes a hole in the lesser omentum and passes a gauze strip or rubber tube, prepared in advance by the sister, around the stomach. A clamp is placed on the ends of this tube or ribbon, which is passed to a second assistant to hold the stomach in an elevated position. The surgeon completes mobilization in the duodenum area. The instruments are supplied in the same sequence: a clamp for separating tissue, two clamps for clamping the resulting portion, scissors for crossing it and two ligatures of the appropriate caliber and material - in each specific case, the surgeon usually names the item he needs. - Crossing the duodenum and processing its stump
. Before crossing the duodenum, the nurse gives the surgeon 2 strong clamps, which he places on the intestine. A crush clamp (or small Payra clamp) is applied closer to the pylorus. To isolate adjacent tissues, the nurse provides two medium napkins, which the surgeon and assistant place around the circumference of the duodenum; prepares a scalpel, a stick with iodine and, at the request of the surgeon, gives him a scalpel, and the assistant - a stick with iodine. The surgeon crosses the duodenum between the clamps (Fig. 89, b), the assistant turns the stomach upward and closes the crossed surface first with the middle one, then wraps a large napkin around the clamp and, finally, fixes it all with a long silk No. 8 ligature. Without any reminders, the operating nurse must quickly provide the materials needed to cover the dirty surface. The contaminated scalpel is put aside on a special napkin: 6N will be needed to cut the stomach. After this, the surgeon begins to process the duodenal stump. In a typical case, it is necessary to apply a long thread of catgut No. 4 on a round intestinal needle. The surgeon places a continuous wrapping suture around the clamp. After applying the suture, the clamp is removed, the thread is tightened, tied and, without cutting off its ends, a second row of interrupted silk sutures No. 4 is applied on the same needle. Before applying the last sutures of the second row, the ends of the catgut thread are cut off. Sometimes the surgeon finds it necessary to apply a third row of sutures - also interrupted with silk No. 2. After suturing the duodenal lumen, wash your hands, change napkins and instruments. In technically difficult cases, the duodenal stump is sutured atypically and the nurse follows the surgeon’s instructions. In any case, she must remember that processing the duodenal stump is one of the critical moments of the operation, and carefully check the strength of the suture material and the serviceability of the instruments before submitting them to the surgeon. - Ligation of the left gastric artery.
An equally important step is the ligation of a large vessel approaching the lesser curvature of the stomach from above and the posterior left gastric artery. If the ligature slips or the hemostat malfunctions, severe arterial bleeding occurs, which is extremely difficult to stop. The nurse should be extremely attentive at this stage, have long hemostatic clamps and an electric suction ready.Rice. 89. Stages of gastric resection according to Finsterer. a-mobilization of the stomach; b — intersection of the duodenum;
Having mobilized the stomach along the lesser curvature, the surgeon incises the anterior layer of the lesser omentum with a scalpel, passes a clamp under the control of a finger through the entire thickness of the omentum and prepares to clamp the artery. At his direction, the sister applies two strong, sharply curved clamps (many people successfully use Fedorov clamps for the renal pedicle for this purpose; see page 21). The left gastric artery, together with the surrounding tissue, is crossed between the clamps. The sister immediately gives another clamp, which is applied to the visible central end of the crossed vessel. To bandage it, use a long (30-40 cm) ligature made of silk No. 6. After tying, its ends are cut off with scissors and the artery is ligated a second time under a clamp applied to the vessel. Silk No. 4 is used here. The part remaining on the stomach is ligated with silk No. 6.
- Preparing a loop of the small intestine for anastomosis with the stomach - see section “Gastroenteroanastomosis”
(section 2a). - Cutting off the stomach, treating the lesser curvature.
The surgeon applies stay sutures using two long silk No. 2 threads on a round needle. Clamps are applied to the holders. After this, a Payr's press and two strong Kocher clamps are applied to the resection line. The abdominal cavity is isolated with napkins, the stomach is cut off with a scalpel along the upper edge of Payra's pulp (Fig. 89, c) and thrown away along with the instruments and scalpel placed on it. The stump is treated with iodine and sutured from the lesser curvature under Payr's sphincter, not reaching the greater curvature at a distance equal to the width of the future anastomosis. The suture is applied with a continuous catgut thread No. 4 on a round needle. Some surgeons prefer to sew not with a curved needle on a needle holder, but with a straight needle, holding it with their fingers.Rice. 89. c - cutting off the stomach; d — application of gastroenteroanastomosis
After applying a continuous catgut suture, the ends of the tied thread are cut off, Payra's sphincter is removed and a second row of interrupted silk sutures No. 2 is applied. The threads of three to four sutures closest to the site of the future anastomosis can be used to fix the afferent loop of the intestine, so they are not cut off, but put a clamp on them.
- Gastroenteroanastomosis.
The sequence of this stage of the operation is described in paragraph 3 of the section “Gastroenteroanastomosis”. The first moment of this stage is the application of interrupted sutures made of silk No. 2 on the posterior lip of the anastomosis, without even opening the lumen of the stomach and intestines (Fig. 89, d). After applying this series of sutures, fixing the posterior wall of the gastric stump to the site of the small intestine selected for anastomosis, the nurse gives the surgeon scissors to cut off all threads except the outer ones, and a scalpel to cut off the gastric stump between the suture line and the clamp remaining on the stump from the side of the greater curvature . In parallel, the lines of applied sutures open the lumen of the small intestine. Using a round intestinal needle, a long (40-50 cm) thread of catgut No. 2 is fed to apply a continuous suture first to the posterior and then to the anterior wall of the anastomosis. To dry the suture line, the assistant is given anatomical tweezers and small balls. After tying and cutting off the ends of the catgut thread, the hands are treated, napkins and tools are changed. The surgeon begins to apply a second row of sutures on the anterior wall of the anastomosis (no. 2 silk threads 16-20 cm long). The anastomosis is completed by fixing the afferent loop of the small intestine above the anastomosis to 3-4 sutures previously placed on the stomach for the purpose of suturing the lesser curvature. The nurse hands the surgeon a needle holder with an uncharged needle; the threads, taken on a clamp, are sequentially threaded into a needle and they are used to suture the intestine to the stump of the stomach. - The final stage of the operation.
After performing the anastomosis, the surgeon fixes the stomach stump to the edges of the window in the mesentery of the transverse colon with 3-4 interrupted sutures made of silk No. 2. The nurse carefully counts the instruments and material used. All holders are cut off, the condition of the duodenal stump is checked again (abdominal speculum may be needed), the tampons are removed from the abdominal cavity, hemostasis is checked and the abdominal cavity is drained. - Suturing a wound of the anterior abdominal wall.
Gastric resection according to Billroth I
Stages 1, 2, 3 are the same.
4. Transection of the duodenum
performed in the same sequence as during resection according to Billroth II. After wrapping the crossed surface of the stomach with napkins and retracting it to the upper corner of the wound, the surgeon does not suture the duodenal stump, but leaving a clamp on it, also closes it with a napkin in order to return to this area after removing the resected part of the stomach and prepare the stump for anastomosis with the remaining part of it.
5. Ligation of the left gastric artery
- see paragraph 5 of the section “Resection of the stomach according to Billroth II”.
6. Cutting off the stomach for treatment of the lesser curvature
- see paragraph 7 of the section “Resection of the stomach according to Billroth II”.
7. Gastroduodenoanastomosis
. Under a clamp applied to the duodenum, the surgeon uses a scalpel to incise the seromuscular membrane, stitches the vessels present here with thin catgut threads on an intestinal needle, ties the threads and cuts them off with scissors. The stomach stump is prepared in a similar way. After this, the surgeon sews together the posterior walls of the stomach and duodenum with interrupted sutures using silk No. 2; the ends of the threads are cut off.
The edges of the duodenum and stomach stumps are cut off with scissors under clamps. At this stage of the operation, an electric suction may be needed. The nurse applies a long catgut thread (No. 4) on an intestinal needle to apply a continuous suture first to the posterior and then to the anterior wall of the anastomosis. The assistant uses anatomical tweezers to dry the suture line with small balls. After tying, the ends of the thread are cut off with scissors.
Change napkins, tools, wash hands.
Interrupted silk sutures are placed on the anterior wall of the anastomosis. Silk threads No. 2 should be 25-30 cm long.
8. The final stage of the operation.
Wipes and instruments are removed from the abdominal cavity, carefully counting them. Toilet the abdominal cavity.
9. Layer-by-layer suturing of the wound of the anterior abdominal wall
.
Gastric resection using staplers
Stages 1, 2, 3 are the same.
4. Transection of the duodenum
. The surgeon places the UKL-40 device on the intended line of intersection of the duodenum, fixes it by tightening the screw until the marks align, and stitches the duodenum with staples (for more details on the procedure for working with the devices, see page 173). A crushing clamp is applied above the apparatus. After isolating the surgical field with napkins, the operating nurse gives the surgeon a scalpel, with which he crosses the duodenum between the UKL-40 and the clamp. Next, the pyloric part of the stomach is treated with iodine and wrapped in napkins. The UKL-40 fixing screw is loosened and the device is removed; the duodenal lumen is sutured with one row of tantalum staples.
For Billroth II resection, one or two rows of silk sutures are placed over the staples.
During Billroth I resection, the seromuscular layer is incised below the line of staples, the vessels are ligated, and before applying the anastomosis, the stitched edge of the duodenum is cut off along with the staples.
5. Ligation of the left gastric artery.
6. Preparation of a loop of the small intestine for anastomosis with the stomach
- see paragraph 6 of the section “Resection of the stomach according to Billroth II”.
7. Cutting off the stomach, treating the lesser curvature.
To treat small curvatures, UKL-60 and UKZH-8 devices can be used.
UKL-60 device
applied from the lesser curvature side together with a crushing clamp and fixed in this position. The surgeon stitches the stomach wall with staples and cuts off the resected part below the applied device. The latch is loosened, the device is removed; the slight curvature is stitched with one row of tantalum brackets. Next, seromuscular interrupted silk sutures are applied, immersing a series of metal staples inside. Anastomosis of the gastric stump with a loop of the small intestine or duodenum is usually performed.
Apparatus UKZH-8
allows you to apply a double-row immersion suture using U-shaped tantalum staples. After mobilization of the stomach, a device with separated halves is applied to its wall from the side of the greater curvature. After checking the correct installation of the device, bring its halves together by rotating the steering wheel. After this, fixing needles are inserted into the holes of the ribs. Raising and lowering the lever of the sewing mechanism, one staple is pushed out of the staple grooves, thus applying stitches.
To insert the first row of sutures and apply a seromuscular suture, both halves of the apparatus are slightly separated. The nurse hands over the immersion machine, which the surgeon uses to immerse the first row of sutures. The second row of sutures is placed using a sewing mechanism located on the machine closer to the remaining part of the stomach. After this, the fixing needles are removed, the central screw is unscrewed, the halves of the apparatus are separated and the plunger is removed. The surgeon removes the device and hands it to the nurse.
Anastomosis of the remaining gastric stump with the small intestine or duodenum is performed in the usual way.
Stages 9 and 10
- as with conventional resection.
Gastrectomy
- Upper-median laparotomy
. - Revision of the abdominal organs.
- Mobilization of the stomach is carried out within a wider range
than resection, but the principle is the same. After crossing the portions of the omentum and ligaments that fix the stomach, on which clamps are applied, reliable ligatures are used (catgut for the remaining part in the body, silk for the part that is removed). - Crossing the duodenum
and suturing its stump can be done manually or using devices (see “Resection of the stomach”). - Mobilization of the left lobe of the liver
, intersection of the branches of the vagus nerve. The area of the cardia and the abdominal segment of the esophagus can be well examined and mobilized only after crossing the triangular hepatophrenic ligament and mobilizing the left lobe of the liver and retracting it to the right (Fig. 90). To do this, you need to submit the longest abdominal mirrors, long clamps and long scissors.Rice. 90. Dissection of the triangular ligament of the left lobe of the liver
The right trunk of the vagus nerve, passing along the posterior right edge of the esophagus, and the left trunk, passing along the anterior left edge, are divided with scissors at the edge of the diaphragmatic opening. The branches of the nerve are always accompanied by blood vessels, for ligation of which it is necessary to apply long catgut threads No. 2-3. In this case, it is convenient for the surgeon to use a special vascular fork to apply ligatures (see page 172).
- Preparation of a loop of small intestine for anastomosis
. The surgeon dissects the avascular zone in the mesentery of the transverse colon and passes the loop of small intestine selected for anastomosis high to the intersection of the esophagus. - Transection of the esophagus
. The surgeon places a soft, curved clamp on the esophagus. For this purpose, a clamp is used to hold the stump of the bronchus or cardiac auricle (Fig. 91). The use of this clamp not only prevents the leakage of esophageal contents, but also fixes the esophagus in a retracted position and assists in suturing. A Fedorov renal clamp is applied to the removed part (see page 21) and the esophagus is cut between the clamps. - Imposition of esophageal-intestinal anastomosis
. The top of the small intestinal loop is brought under the esophageal stump and the first row of interrupted silk sutures is placed on the posterior wall of the anastomosis. At the same time, the sister feeds silk No. 2 threads 40-50 cm long on a round intestinal needle. The ends of the threads are not tied until all the stitches have been placed. The second row of interrupted sutures is applied on the same needle with the same long catgut threads No. 2 (Fig. 92). The anterior wall of the anastomosis is formed in the same way as the posterior one. - Application of intercervical anastomosis
. A side-to-side anastomosis is performed between the afferent and efferent loops (see page 139). - Fixation of loops in the window of the mesentery of the transverse colon.
- Suturing a wound of the anterior abdominal wall.
Rice. 91. Soft crank clamp for esophageal stump
Rice. 92. Applying an internal row of sutures to the posterior wall of the esophageal-intestinal anastomosis
Gastrectomy using staplers
Stages 1, 2, 3 are the same.
4. Transection of the duodenum
. For this purpose, UKL-40, UKL-60 devices can be used.
Stages 5, 6 and 7 are the same.
8. Establishment of esophageal-intestinal anastomosis using the PKS apparatus.
Having removed the mushroom with the rod from the apparatus, the tubular body is inserted through the intestine by cutting it at a distance of 12-15 cm from the site of the anastomosis. In the intestinal wall at the site of the anastomosis, the surgeon makes a puncture with a scalpel through which a rod with a mushroom is inserted into the body of the apparatus. Then the fungus is introduced into the stump of the esophagus, onto which a purse-string suture is first applied. After tightening the purse-string suture around the rod, the fungus is brought closer to the apparatus body by rotating the nut so that the sutured tissues of the esophagus and intestines are located between the apparatus body and the mushroom. After removing the fuse, stapling occurs by squeezing the handles of the device until it stops. By turning the nut 1-2 turns counterclockwise, the tissues compressed between the body and the mushroom are released and the apparatus is removed from the intestine. After this, additional seromuscular interrupted silk sutures are manually applied around the entire circumference of the anastomosis. The defect in the intestinal loop, located 12-15 cm from the anastomosis, is either sutured with a double-row suture, or used to apply a side-to-side interintestinal anastomosis.
Stages 9, 10 and 11 are the same.
Operation technique
Carrying out gastric resection is a technically complex process, and in order to avoid postoperative inflammation, scarring and other complications, you should take seriously the choice of a medical institution and the qualifications of surgeons. The choice of surgical technique depends on the degree of organ damage, the patient’s condition, his age, anatomical and other characteristics. All types of resection are performed under general anesthesia, and the duration of surgical intervention on the stomach does not exceed three hours.
Basic methods of performing the operation
There are many different options for gastric resection and reconstruction. Theodor Billroth first performed such an operation back in 1881, and in 1885 he also proposed another way to restore the functioning of the gastrointestinal tract. These gastric surgeries are still used today, but today they have been modernized and simplified, so they are available to a wide range of practicing surgeons. The doctor selects the type of operation individually in each case, but more often they use:
- Subtotal distal resection, when the lesion is located in the pyloroantral part of the lower third of the stomach (the entire lesser curvature).
- Subtotal proximal resection, performed for stage 1 and 2 gastric cancer, when the lesser omentum, lymph nodes, lesser curvature and a section of the greater omentum are removed.
- Gastrectomy, which is performed in the presence of a primary multiple tumor or infiltrative cancer located in the middle part of the stomach. The entire organ is removed, and an anastomosis is performed between the esophagus and the small intestine.
By Billroth 1
Gastric resection according to Billroth 1 is the excision of 2/3 of the organ, when the physiological path of food movement with the participation of pancreatic excretion and bile is preserved. During surgery, the anastomosis of the duodenum and stomach is connected end to end. This method is used for polyps, malignant ulcers, and small cancerous tumors of the gastric antrum.
- Differences between coughs during Covid and influenza or acute respiratory infections
- Plum compote for the winter recipes for a 3 liter jar
- Tax deduction 50 thousand rubles. for pensioners
By Billroth 2
During Billroth 2 resection, a large part of the blind stump of the duodenum and stomach, anterior and posterior anastomosis (connection of two organs) are removed. After this operation, the physiological path of food movement is disrupted - it enters directly into the jejunum, and bile reflux is possible and the anastomosis is disrupted. Resection according to Billroth 2 has more indications, since it is performed on gastric ulcers of any location and for cancer, since it gives the doctor the opportunity to perform extensive removal of the organ up to 70%.
According to Hoffmeister-Finsterer
The Hofmeister-Finsterer technique is a modified version of Billroth 2, which provides for resection of at least 2/3 of the organ for peptic ulcer disease. During the operation, the entire secretory zone is removed, after which the motor function of the stomach undergoes significant changes: peristalsis weakens, the function of the pylorus, which ensures the gradual evacuation of food, disappears altogether.
By Ru
The Roux method is the removal of part of an organ with a Y-shaped gastroenteroanastomosis. In this case, the jejunum is divided, and its distal end is sutured and connected to the lower third of the gastric stump. This is also a modification of Billroth 2, which is indicated for duodenogastric reflux esophagitis, which is characterized by the reflux of the contents of the duodenum into the stomach.
According to Balfour
The Balfour method involves placing a gastrointestinal connection on a long loop of jejunum. This method prevents pathological changes in the organs of the gastrointestinal tract, and is also used for very high resection due to peptic ulcer or the impossibility of suturing in another way due to the anatomical features of the gastric stump. Balfour resection eliminates the gap between the knees of the jejunum, which eliminates the future occurrence of intestinal obstruction.
Gastric resection according to Billroth 2: surgical technique, complications
Gastric resection according to Billroth 2 is an abdominal surgery operation that is performed for the treatment of cancer and complicated peptic ulcers. The essence of the operation is to remove a significant part of the organ and create an anastomosis between the stump and the jejunum. The technique has a number of disadvantages and is used when it is impossible to use another surgical technique.
Billroth resection 1, 2: history
The first gastric resection with the creation of a gastroenteroanastomosis was performed in 1881 by the outstanding Austrian physician Theodor Billroth. The indication for surgery was oncological disease (stomach cancer). During the procedure, a unique surgical technique was used at that time with the creation of end-to-end gastroduodenoanastomosis. Later this technique became known as Billroth 1.
In 1885, Theodor Billroth proposed a second method of creating an anastomosis between the stump and the lower parts of the digestive tract - side-to-side gastrojejunal anastomosis. The anastomosis connected the stump of the stomach and the loop of the jejunum. The part of the small intestine located above the anastomosis and including the duodenum was sutured. This version of the surgical manual is called Billroth 2.
Resection according to Billroth 2 has objective disadvantages, which are described in the corresponding section of the article. The disadvantages of the method forced surgeons to look for other options for creating an anastomosis. Today, there are many modifications of the Billroth 2 technique, among which the Hoffmeister-Finsterer method and Roux-en-Y resection are the most widespread.
Indications for surgery
Billroth 1, 2 - abdominal surgery operations, in which the distal part of the stomach is removed, followed by the creation of an anastomosis between the stump and the lower parts of the small intestine.
Indications for removal of part of the stomach are:
- Oncological disease.
- Benign tumor.
- Peptic ulcer with complications.
The Billroth gastrectomy technique is also used in the treatment of severe abdominal injuries. In bariatrics (obesity surgery), Billroth surgical procedures are not used. To treat obesity and accompanying diseases of the endocrine and cardiovascular systems, a special technique is used - longitudinal resection, also known as sleeve gastroplasty.
Longitudinal resection does not disrupt the natural passage of food through the gastrointestinal tract and is free from all the disadvantages inherent in the methods discussed in this article.
Types of gastric resection
Depending on the location of the pathological focus, as well as the goals and objectives of the operation, the surgeon performs distal, antral, proximal, subtotal, total or longitudinal resection of the stomach.
Distal
resection
is a classic abdominal surgery procedure in which the doctor removes 60% to 75% of the distal part of the stomach. The proximal cardiac portion remains and is used to create the anastomosis. Distal gastrectomy is used for benign tumor processes and in the treatment of oncological diseases.
Antral resection
- a variant of the operation in which the surgeon removes only the antrum of the organ, that is, approximately one third of the stomach. Antral gastrectomy is used mainly in the treatment of peptic ulcers and benign diseases.
Proximal resection
- removal of the upper part of the organ bordering the esophagus. Proximal gastrectomy is used for tumor processes in the cardiac part of the stomach.
Subtotal resection
- a large-scale operation during which more than 80% of the organ is removed. Subtotal gastrectomy is used in the treatment of cancer. According to statistics, at least 60% of patients with malignant neoplasms require subtotal resection, since only this can minimize the risk of tumor spread to the lymph nodes and neighboring organs.
Total resection
- removal of the entire organ. Total gastrectomy is used for cancer.
Longitudinal resection
— removal of part of the organ along the greater curvature with complete preservation of the lesser curvature, cardiac part and pylorus. This surgical option is used in the treatment of obesity and obesity-associated chronic diseases. The goal of surgical treatment is to reduce the volume of the organ to reduce food intake.
Billroth 1, 2: surgical technique
Resection of a part of an organ is the first stage of surgery. In the second stage of gastrectomy, the surgeon restores the integrity of the digestive tract by creating a connection (anastomosis) between the stump and the small intestine. Billroth 1 and 2 are various surgical aids (techniques) used in the formation of anastomosis.
Gastric resection according to Billroth 1
is
an operation in which an anastomosis connects the stomach to the duodenum and is created end-to-end. What does this mean?
The surgeon sutures the stump from the lesser curvature side, leaving a small area open in the area of the greater curvature. The open terminal portion (end) of the gastric stump is connected by a muscular suture to the end of the duodenum. This is how gastroduodenoanastomosis according to Billroth 1 is formed.
Gastric resection according to Billroth 2
- an operation in which an anastomosis connects the stump of the stomach with the jejunum. The duodenum is sutured and excluded from the passage of food, which is the main disadvantage of the technique and causes the development of postoperative complications.
A loop of jejunum is brought into the upper floor of the abdominal cavity through an opening in the mesentery of the colon. A hole is created in the side of the intestine, which is sutured to the side of the stomach stump along the greater curvature. Along the lesser curvature, the gastric wall is sutured tightly. A gastrojejunostomy is formed, the stomach and intestines are connected side to side.
Hoffmeister-Finsterer technique.
This surgical manual is a modification of the Billroth operation 2. The fundamental difference between gastric resection according to Hoffmeister-Finsterer is that the end section of the stomach stump is sutured to the side hole in the wall of the jejunum, that is, an anastomosis is formed according to the end-to-side principle. The part of the intestine located above the anastomosis is sutured to the stump from the lesser curvature. The duodenum is sutured and excluded from the passage of the food bolus.
The Hoffmeister-Finsterer method can significantly reduce the risk of developing postoperative complications characteristic of Billroth-2 gastrectomy. But part of the jejunum and duodenum is still excluded from the digestion process, which can lead to the development of complications. To eliminate this drawback, Roux-en-Y surgery has been proposed.
Resection according to Roux
. The peculiarity of the Roux-en-Y surgical manual is that the anastomosis between the jejunum and the stump is formed according to the end-to-end principle. To do this, the small intestine in the upper section is cut into two parts.
The distal end of the jejunum is connected to the stump using muscle sutures. A gastrojejunal anastomosis is formed, connecting the stump to the intestine. The proximal end of the jejunum, which is anatomically connected to the distal duodenum, is sutured to the intestine below the anastomosis. The proximal part of the duodenal stump is sutured.
This principle of reconstruction of the upper gastrointestinal tract makes it possible to avoid the reflux of gastric contents through the anastomosis into the duodenum. There is no risk of stagnation and rotting of fragments of the food bolus in the duodenum, there is no risk of failure of the sutures of the duodenum, duodenogastric reflux and other postoperative complications of the Billroth 2 operation.
Comparison of operations: advantages and disadvantages
Billroth resection 1 is an abdominal operation with minimal, as far as possible in this situation, changes in the physiology and anatomy of the upper gastrointestinal tract. In simple terms, this is the best of the methods considered. Its advantages:
- The natural passage of the food bolus through the duodenum is preserved.
- End-to-end anastomosis allows the reservoir function of the gastric stump to be preserved to the maximum extent.
- There is no direct contact of gastric juice with the epithelium of the jejunum, which minimizes the risk of developing peptic ulcers of the anastomosis.
- The risk of developing dumping syndrome is significantly lower. There is virtually no risk of developing a severe form of dumping syndrome.
- There is no risk of developing afferent loop syndrome.
In the case of gastric resection according to Billroth 2, for all the five points discussed above, we see the opposite picture. Disadvantages of this surgical manual:
- The bolus of food enters directly into the jejunum, which is not physiological.
- The reservoir function of the gastric stump is reduced, food enters the intestines faster.
- Gastric contents come into contact with the jejunal mucosa, which increases the risk of developing a peptic ulcer of the anastomosis.
- There is a high risk of dumping syndrome (develops in 20-50% of patients), including severe forms.
- There is a high risk of afferent loop syndrome.
The Billroth-2 technique is imperfect. It is used when it is impossible to create gastroduodenoanastomosis according to Billroth 1 due to the risk of excessive tension of the duodenum (fraught with failure of the muscle sutures). If it is possible to use the modified Hoffmeister-Finsterer technique or the Roux-en-Y procedure, one of these surgical techniques is chosen. If this is not possible, Billroth 2 surgery is performed.
Complications after Billroth 2
Dumping syndrome
. One of the most common complications of gastric resection according to Billroth 2 is dumping syndrome. According to statistics, it occurs in 20-50% of patients who have undergone surgery.
Dumping syndrome develops due to too rapid entry of the food bolus into the jejunum. Undigested food has mechanical, osmotic and chemical properties unfavorable for the intestines. Irritation of the mucous membrane of the jejunum is accompanied by a sharp increase in blood circulation in the intestinal vessels, which in turn leads to hypovolemia (decrease in circulating blood volume) and deterioration of blood circulation in the central nervous system.
Dumping syndrome manifests itself in attacks with deterioration of well-being, dizziness, shortness of breath, tachycardia and other symptoms. The attack begins 10-20 minutes after eating. It is usually provoked by dairy products and simple carbohydrates. In severe forms of the syndrome, any food acts as a provoking factor.
Mild and moderate forms of dumping syndrome are treated conservatively, with the help of diet and drug therapy aimed at slowing down the evacuation of the food bolus and accelerating the digestion of the food bolus in the stomach.
In severe cases, reconstructive surgery is performed to create a gastroduodenoanastomosis according to Billroth 1 or a gastrojejunostomy according to Roux. The operation is also indicated for patients with moderate dumping syndrome when conservative treatment is ineffective.
Adductor loop
syndrome . The cause of the complication is duodenogastric reflux, that is, the reflux of the contents of the duodenal stump through the anastomosis into the stomach stump. During an attack, the patient’s well-being sharply deteriorates, belching, heartburn, and severe nausea appear. At the peak of the attack, vomiting occurs, which brings instant relief. Vomit contains large amounts of bile.
Adductor loop syndrome is often accompanied by duodenostasis (stagnation of contents in the lumen of the duodenal stump), impaired liver function, jaundice, and inflammation of the pancreas. The patient should immediately contact their doctor when the first signs of this complication appear.
Treatment of mild and moderate forms of this complication is based on conservative methods. Surgical treatment with reconstruction of the gastrojejunal anastomosis into enteroenteroanastomosis according to Brown. Reconstructive surgery is also indicated for moderate severity of afferent loop syndrome, if conservative treatment is ineffective.
Peptic ulcer of the anastomosis.
The mucous membrane of the jejunum is unstable to aggressive gastric juice. Direct contact of the stomach contents with the intestinal epithelium, which occurs after the Billroth 2 operation, leads to the development of inflammation with the appearance of erosions and ulcers in the anastomotic area.
This complication is treated conservatively. Drug therapy is carried out in combination with diet, aimed at reducing the acidity of gastric juice. If conservative therapy is ineffective, the question of surgical treatment using vagotomy or reconstructive surgery is raised.
Atrophic gastritis
. Several pathogenetic factors are present in the development of inflammation of the gastric mucosa. Distal gastrectomy is performed with the removal of the antrum, in which gastrin is synthesized, a hormone that affects gastric secretion.
Many patients after resection according to Billroth 2 have duodenogastric, biliary and intestinal reflux to varying degrees. Intestinal contents, which normally do not enter the stomach, provoke atrophic and inflammatory changes in the mucosa.
Atrophic gastritis manifests itself as heaviness in the epigastrium, moderate nausea, loss of appetite, heartburn, and belching. Patients gradually lose weight. General health deteriorates, and anemia develops due to impaired synthesis of the internal Castle factor.
Treatment of atrophic gastritis is conservative. It is important to follow a therapeutic diet with frequent split meals. Patients are prescribed anabolic drugs; to prevent anemia and asthenia, injections of B vitamins are prescribed. For low acidity, gastric juice and digestive enzymes are indicated; for high acidity, H2 receptor blockers are prescribed.
You can get more information about abdominal and bariatric surgery at a consultation with a doctor at the Weight Loss Center clinic. Branches of the medical center are located in St. Petersburg and Sestroretsk.
Rehabilitation process after surgery
As after any surgical intervention, so after gastrectomy, all sorts of complications and risks of developing negative symptoms arise: peritonitis, bleeding, anemia, reflux esophagitis, dumping syndrome. The average length of a patient's stay in the hospital after surgery is from 2 to 3 weeks, and the patient can sit as early as 5-6 days after resection. According to the doctor's recommendation, physical activity should be limited for some time, and a bandage should be worn for 4-6 months. Complete restoration of gastrointestinal functions occurs after 3-5 years.
Diet and nutrition after resection
After removal of part of the stomach, nutrition must be adjusted, because food very quickly after resection comes from the esophagus into the small intestine, so complete absorption of nutrients will not always occur during meals. The following nutritional rules will help you avoid complications after gastric surgery:
- eat up to 6 times a day;
- eat slowly, chewing food thoroughly;
- limit dishes containing easily digestible carbohydrates: honey, sugar, jam;
- tea, milk, kefir and other drinks should be consumed no earlier than 30 minutes after meals, so as not to overload the stomach;
- Particular importance should be given to animal proteins, which are found in chicken, eggs, fish, cheese, cottage cheese and vitamins contained in vegetables, fruits, berries, and herbal infusions.
In the first 3 months after resection, special emphasis should be placed on nutrition, because at this time the digestive system adapts to new living conditions. At this time, you should eat mainly mashed or chopped steamed foods. Recommended dishes: vegetable broth soups, pureed milk porridges, vegetable soufflés, fruit puddings, steam omelettes, whole milk, sour cream sauces, weak coffee with cream and tea with milk.
Sample menu
In the first days after resection it is recommended:
- Day 1: complete fasting;
- Day 2: fruit jelly, unsweetened tea, still mineral water, 30 ml every 3 hours;
- Days 3 and 4: soft-boiled egg, 100 ml of unsweetened tea, rice porridge, meat cream soup, rosehip decoction, curd soufflé;
- Days 5 and 6: steam omelette, milk tea, pureed buckwheat porridge, pureed rice soup, steamed meat dumplings, carrot puree, fruit jelly;
- Day 7: liquid rice porridge, 2 soft-boiled eggs, sugar-free cottage cheese soufflé, pureed vegetable soup, steamed meat cutlets, steamed fish fillet, mashed potatoes, jelly, white bread crackers.