Material tested:
Kravchenko Boris Sergeevich, surgeon - 12/24/2019
The pathology in question is a very popular phenomenon among the population, which cannot be called dangerous, but the treatment of which takes a lot of time. In some cases, this defect is discovered by chance, when there are no complaints from patients.
In other situations, ignoring the disease provokes the emergence of a new, more serious pathology: chronic or acute cholecystitis, biliary dyskinesia.
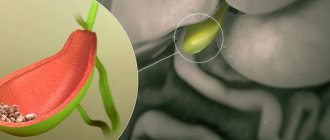
What is gallbladder constriction?
CT scan of gallbladders with constrictions
Constriction of the gallbladder is a negative change in the shape of the organ.
A congenital constriction is formed in a child as a result of development in the womb. This occurs in the fifth or sixth week during the development of the digestive tract organs. The congenital disease does not cause any special sensations or complications. There is a possibility that the pathology will disappear as you grow older. However, for certain reasons, cholelithiasis or pericholecystitis may occur.
Acquired constriction of an organ occurs in a person in adulthood or old age. The disease is dangerous because it causes stagnation of secretions and occasionally leads to the death of cells on the walls of the internal organ.
Products prohibited for 1.5 months
For one and a half months after gallbladder removal, you should not eat the following foods:
- fresh vegetables and fruits;
- fresh bread white bread;
- rye bread of any age;
- crumbly porridge;
- easily digestible carbohydrates (sweets, honey, sugar).
The last limitation is related to the prevention of bile stagnation.
Fatty, salty, spicy, smoked dishes are certainly prohibited, and not only during this period, but also in the subsequent menu throughout the year.
Food must be thoroughly chopped; it should not be cold or too hot.
Etiology of the disease
The acquired constriction appears during the life cycle. Its formation is provoked by the following reasons:
- the presence of adhesions on the walls of the organ resulting from the inflammatory process;
- omission of other internal organs that produce compression;
- stone formation;
- an increase in the size of the liver that occurs due to various pathologies;
- constant intense physical activity, including lifting heavy objects;
- prolonged fasting followed by overeating;
- sudden weight gain;
- unbalanced diet, strict diets and long-term consumption of junk food;
- frequent nervous tension, stress, accompanied by eating a large amount of food.
Sometimes doctors associate the occurrence of organ constriction with pathologies of other organs of the gastrointestinal tract.
Pregnant women are at risk, since during pregnancy there is a possibility of compression and displacement of internal organs.
People who are often in a sitting position are more susceptible to the disease. Sedentary work increases the risk of constriction.
Watch the video to see how fasting affects the gallbladder:
What can you eat for the first 45 days?
After laparoscopy
the patient receives general nutritional advice.
Strict adherence to the diet is prescribed for the entire first year after surgery, until the restructuring in the body is completed.
Even after gentle laparoscopic surgery, the patient remains in intensive care for 24 hours.
At this time, eating is excluded, you can only drink a small amount of water. Over the next month and a half, the diet changes day by day:
| Period | Recommendations | Rules for eating |
| Second day after surgery |
|
|
| 3 – 5 days |
|
|
| Day 6 and 7 |
| The diet remains the same. |
If the recovery period is favorable, on the 8th day the patient is transferred to a special diet - table No. 5. Diet numbers can vary - 5A, 5B, 5Sh, 5P, depending on the presence of concomitant pathology or complications that have arisen.
From the eighth day to one and a half months, nutrition remains as gentle as possible. Meat dishes should be served only in the form of minced meat - meatballs, meatballs, steamed cutlets. Soups should be pureed. Puddings, soufflés, casseroles are recommended. Slimy porridges (oatmeal), jelly and non-acidic juices are useful.
Clinical picture of gallbladder constriction
The congenital disease often goes away without symptoms. The problem is discovered accidentally during an ultrasound examination. If the constriction is strong, then when transferring the baby to solid food, the following may occur:
- nausea;
- periodic pain in the peritoneum;
- gagging.
Often such symptoms are mistaken for a gastrointestinal disorder.
A disease acquired during life sometimes also occurs without symptoms, but more often it still has a certain clinical picture. With prolonged stagnation of bile or the onset of the inflammatory process, the following signs will make themselves felt:
Excessive sweating may be a symptom of gallbladder constriction
- vomiting attacks, accompanied by the release of a certain amount of bile;
- yellowness of the skin and sometimes mucous membranes;
- bitter taste in the mouth;
- severe pain on the right side under the ribs;
- change in the color of stool, becoming colorless;
- the presence of dark-colored urine;
- loss of appetite and weight loss;
- profuse sweating;
- bowel disorder, most often characterized by diarrhea;
- yellow or white coating on the tongue;
- heaviness and unusual sensations in the stomach.
Rare symptoms are:
- loss of consciousness;
- transfer of pain from the peritoneum to the back;
- elevated temperature.
Symptoms
During the initial stage of constriction formation, the patient's condition worsens. He may attribute this to gastrointestinal problems or fatigue from work. Next, pathological symptoms appear, due to which the doctor prescribes instrumental and laboratory research methods to make a diagnosis.
Possible:
- Dyspeptic disorders. The condition begins with nausea, which intensifies after vigorous physical activity or eating. When the maximum peak of the inflammatory process is reached, the patient vomits. It appears during severe inflammatory processes, when the outflow of bile is obstructed.
- Pain syndrome. The unpleasant sensation is localized in the area of the right rib. But the patient may mistake it for liver disease. The cause of pain is stretching of the walls, accumulation of secretions that cannot come out. Also, sensations appear when stones accumulate, which with sharp edges injure the mucous membrane.
- Intoxication. Formed due to the development of bile peritonitis. Severe fatigue, headache, muscle aches, and dizziness appear. Body temperature rises, which is accompanied by increased pain.
- Changing the stool. The feces become colorless. This condition is formed due to a violation of the outflow of bile, which leads to disruption of the metabolism of bilirubin.
The majority of symptoms also develop in other diseases. Therefore, it is important to make a diagnosis in time. If left untreated, the symptoms of the disease intensify, resulting in acute pain with fever. The main danger is the exacerbation of pathological symptoms during constriction.
Diagnosis of the disease
The following actions help to diagnose gallbladder constriction:
| Initial examination by a gastroenterologist | During the examination, the doctor interviews the patient, identifying the symptoms of the disease. |
| Examination of the patient's body | The doctor palpates the patient's abdominal area and assesses the condition of the mucous membranes and skin. |
| Laboratory examinations | Specialists conduct an analysis of the patient’s blood, urine, and stool to determine the degree of development of the disease and the presence of complications. |
| Ultrasound examination | Using an ultrasound, a specialist determines the thickness of the walls of the internal organ, its size, and the presence of pathology. This study includes several steps. First of all, an ultrasound is performed on an empty stomach after a special three-day diet. The gastroenterologist gives the patient dietary recommendations in advance, and the patient prepares for the ultrasound at home. The second study is carried out half an hour after taking the choleretic medication. |
Treatment of biliary dysfunctions in children
P
The problem of biliary dysfunction, as an integral part of the functional pathology of the digestive tract, is one of the most pressing in gastroenterology. This is primarily due to the difficulties of understanding the term “functional pathology” as such, its debatability, and the lack of uniform clinical and diagnostic criteria and therapeutic approaches.
Currently, dysfunctions of the biliary tract are understood as violations of the motor-evacuation function of the gallbladder, bile ducts and sphincter of Oddi tone, leading to stagnation of bile
[5,7–9,12].
Often, dysfunction of the biliary tract occurs in children with multiple foci of secondary infection, with helminthic infestation, after viral hepatitis, dysentery, with an incorrect daily routine (sedentary lifestyle, overwork at school), disrupted diet (irregular or rare meals at large intervals ), are a consequence of neurosis, force-feeding, conflict situations at school and family [1,4,5].
Dysfunctions of the biliary tract, according to the international classification, are divided into two types: gallbladder dysfunction
and
sphincter of Oddi dysfunction
[3]. There are primary and secondary dysfunctions of the biliary tract [3,6].
To primary biliary dysfunctions
These include diseases that are based on functional disorders of the biliary system due to disorders of neurohumoral regulatory mechanisms, causing disruption of the outflow of bile and/or pancreatic secretions into the duodenum in the absence of organic obstacles [16].
Secondary dyskinesias of the biliary tract
are combined with organic changes in the gallbladder, sphincter of Oddi, or occur reflexively in various diseases of the abdominal organs [13–15].
There are several variants of disturbance of the motor activity of the gallbladder and the sphincter apparatus of the biliary tract: hypotonic, hypertonic and hyperkinetic
. In children with a predominance of the tone of the sympathetic nervous system, hypomotor dysfunctions of the biliary tract are more often observed, and in children with a predominance of the parasympathetic nervous system, hypermotor dysfunctions are observed. However, it should be noted that, given the peculiarity of the physiology of the gallbladder, that is, the impossibility of determining its initial volume due to the constant reabsorption of water from the gallbladder bile, this division has more clinical significance. Patients experience pain resulting from stretching of the gallbladder wall, which contributes to excessive release of acetylcholine, which significantly reduces the formation of cholecystokinin in the duodenum. This slows down the contractile function of the gallbladder [2,5,10,11].
The most accurate method in terms of differentiating various forms of biliary dysfunction is dynamic hepatobilis scintigraphy
, with the help of which it is possible to diagnose initial functional changes in the bile ducts, reflux into the bile ducts, and identify a non-functioning gallbladder.
However, in children, the use of this method is possible only from 12 years of age. Ultrasonography
occupies one of the leading places in the diagnosis of biliary tract pathology .
It allows you to determine the location and shape of the gallbladder, its external contours, the condition of the gallbladder wall, intravesical pathological structures (septa, stones, polyps, etc.), determine the condition of the bile ducts, as well as the liver, pancreas, spleen, and identify “ disabled" gallbladder and the causes of its occurrence [10,14–16]. The method can be used on a child of any age and has virtually no contraindications. Cholecystography
(oral and intravenous)
occupies a prominent place in the diagnosis of biliary tract pathology Currently, fractional duodenal intubation
, which makes it possible to diagnose dyskinetic disorders of the biliary tract organs.
Considering the above, differentiated therapy of biliary dysfunctions is of great difficulty. It is known that the condition for the normal functioning of liver cells, and thereby the entire hepatobiliary system, is the absolute integrity of the membranes and the physiological structure of the cell organelles. Stabilization of cell membranes ensures physiological secretion of bile, and restoration of intercellular connections ensures normalization of its outflow. Therefore, the goal of this work was to develop optimal treatment regimens for biliary dysfunction using the modern multifunctional drug hepabene.
Materials and methods
We observed 130 children from 4 to 14 years old with biliary dysfunction: 30 children from 4 to 7 years old, 50 children from 7 to 10 years old, 50 children over 10 years old.
The diagnosis was based on the results of a clinical examination of patients, laboratory (coprogram, biochemical blood test) and instrumental research methods (ultrasound examination of the liver, gall bladder, pancreas). Patients were diagnosed with concomitant diseases of the digestive system (gastritis, duodenitis, peptic ulcer, functional intestinal disorders).
Research results
The hypertensive form of dysfunction was found in 90 children (69.2%), of which 63 cases (70.0%) were under 10 years of age. The hypotonic form was found in 40 children (30.8%), of which 23 children (57.5%) were older than 10 years. Gallbladder kinks were detected in 41 children (31.5%). Signs of inflammation in the gallbladder were diagnosed in 21 cases (16.2%), of which 13 children (61.9%) were over 10 years old.
Clinically, dysfunction of the biliary tract in children under 7 years of age was accompanied by decreased appetite, bowel dysfunction (mainly constipation), and occasional attacks of nausea. 22 children in this group had abdominal pain, mostly of a paroxysmal nature, usually after eating. In 20 children of this group (66.7%), ultrasound revealed changes in the pancreas (its enlargement, moderate heterogeneity of the echostructure; the appearance of neutral fat). In 11 children of this group, functional changes in the cardiovascular system were revealed, accompanied by muffled heart sounds, a soft systolic murmur of a functional nature, and a decrease in blood pressure. The electrocardiogram (ECG) showed an increase in heart rate, a shortening of the PQ interval, a decrease in voltage, a high, pointed T wave in the 5th and 6th chest leads, a low P wave in the II standard lead.
The data obtained indicate in favor of a syndrome of autonomic dysfunction, against the background of which manifestations of dysfunction of the biliary tract occur. In this case, the predominance of vagotonia is accompanied by a hyperkinetic form of biliary tract dysfunction. In the hypotonic form of gallbladder dysfunction, the pain was often dull and long-lasting.
In children over 10 years of age, against the background of autonomic dysfunction, inflammatory changes in the gallbladder were detected in 13 cases (26.0%), and in 5 cases, pronounced fibrous-focal changes in the pancreas according to ultrasound data, a large amount of neutral fat, iodophilic flora, soap in the coprogram . That is, in children from 7 to 10 years of age, against the background of biliary dysfunction, the risk of developing inflammatory changes in the gallbladder, diagnosed on ultrasound as thickening of its wall and the appearance of sediment in the cavity, increases.
Studies have shown that the development of biliary tract dysfunction in children is closely related to the severity and duration of autonomic dysfunction syndrome
and manifests itself in the form of functional disorders in preschool age, progresses in the early school period, and at the age of over 10 years it is often registered as a chronic disease.
Complex treatment in a day hospital included correction of autonomic dysfunction: limitation of emotional and physical stress, courses of physical therapy, physiotherapeutic treatment, massage of the collar area, water procedures (contrast shower, soothing baths with essential oils of medicinal herbs). Intermittent courses of choleretic therapy were carried out: alternating choleretic drugs and decoctions of choleretic herbs. According to indications, intermittent courses of enzyme therapy and myotropic antispasmodics (duspatalin) were administered.
During the treatment of the hyperkinetic form of biliary dysfunction, sedative and antispasmodic drugs (duspatalin, No-shpa) were used.
If kinks or constrictions of the gallbladder were detected by ultrasound or cholecystography, antispasmodic drugs were prescribed in repeated courses of 10–14 days per month for 3–4 months. In the future, according to indications, the course will be per quarter. Tubage is not shown. Exercise therapy is prescribed after the symptoms of exacerbation have subsided.
For hypotonic forms of biliary tract dysfunction, tubages according to Demyanov were used 2-3 times a week (for a course of 10-12 procedures), combined with taking choleretics 2 weeks a month for six months, tonic physical therapy with a gradual increase in load, physiotherapeutic procedures, vitamins.
We studied the effect of the drug hepabene
on the function of bile formation and bile excretion in biliary dysfunctions in children. The drug was administered to 40 patients from the study group, aged 6 to 14 years, suffering from biliary tract dysfunction.
Depending on the age, the drug hepabene was prescribed in a dose of 1 caps. x 2 times (children from 6 to 10 years old) up to 1 caps. x 3 times (children over 10 years old) after meals for 10–14 days. When analyzing the data obtained, the following was revealed:
- pain disappeared within 3–4 days from the start of taking the drug;
- normalization of stool with a tendency to constipation was noted on days 5–6 from the start of taking the drug;
- in 21 children out of 30 (70%) with decreased appetite, their appetite improved by the end of the 1st week of treatment;
- in the coprogram, the disappearance of fatty acids was noted in 16 children out of 24 (66.7%), where their content was noted from moderate to high quantities;
- fecal neutral fat decreased from moderate to high to negligible in 18 of 26 (69.2%);
- the size of the liver decreased in all children (34 patients), who at the time of admission had an increase from 1.5 to 3.0 cm below the edge of the costal arch;
- a decrease in the size of the enlarged gallbladder was observed in 25 children out of 32 (78.1%) who had an enlargement at the time of admission;
- the presence of sediment in the gallbladder was noted in 12 patients; after 2 weeks from the start of treatment, its disappearance was noted in 3 children (25.0%), which necessitates the need to continue the course of treatment;
- the level of total bilirubin decreased from 14.8±3.8 µmol/l to 7.5±2.3 µmol/l;
- the level of direct bilirubin decreased from 3.5±1.2 µmol/l until it completely disappeared;
- ALT level decreased from 25±5.0 IU/l to 17.0±2.0 IU/l.
Discussion
The results of the studies show that in children with biliary dysfunction, during treatment with the inclusion of the drug hepabene in the therapeutic complex, there is a clinical improvement in the course of the disease, accompanied by a decrease in pain, normalization of stool, improved appetite, and a decrease in liver size. The results of laboratory studies indicated an improvement in coprogram indicators in the form of a decrease in the amount of neutral fat and fatty acids, a decrease in the level of bilirubin and ALT in biochemical blood tests; a decrease in the size of the gallbladder during ultrasound examination in 78.1% of cases, and in some cases, the disappearance of sediment in the gallbladder (in 25% of cases).
During the treatment, the children tolerated the drug hepabene well; no allergic reactions or side effects were detected. However, it is not recommended for patients with Wilson-Konovalov disease as a hepatoprotective agent due to the accumulation of copper in milk thistle, which is an integral part of the drug.
Thus, the herbal preparation hepabene can be recommended for the treatment of biliary dysfunctions in children as a choleretic, antispasmodic and hepatoprotective agent.
Literature:
1. Antropov Yu.F. Neurotic depression in young children. Pediatric gastroenterology 2001. Collection of materials from the 8th conference “Current problems of abdominal pathology in children.” From 29–34.
2. Diagnostic programs for various diseases and physiological norms of the child’s body. (Baranov A.A., Shilyaev R.R., Chemodanov V.V., Baklushin A.E., Bezmaternykh N.A., Lomoskov V.A., Fadeeva O.Yu., Kopilova E.B.) Ivanovo , 1997, p. 83.
3. International Bulletin: Gastroenterology. 2001. No. 5
4. Neudakhin E.V. Pathogenetic role of chronic stress response in the development of abdominal pathology in children. Pediatric gastroenterology 2001. Collection of materials from the 8th conference “Current problems of abdominal pathology in children.” From 10–12.
5. Ursova N.I. Dysfunctional disorders of the biliary tract in children: criteria for diagnosis and correction Consilum. Appendix Pediatrics, 2002, No. 1, p. 23–24
6. Beckingham IJ BMJ 2001; 322:91–94.
7. Corazziari E., Shaffer EA, Hogan WJ at al. Functional disorders of the biliary tract and pancreas.//Gut. – 1999. – Vol. 45 (Suppl. 2). – P. 1148 – 1154.
8. Crawford JM, Gollan JL. Transtranscellular of organic anions in hepatocytes: still a long way to go. Hepatology 1991; 14:192.
9. Cullingford G, Davidson B, Dooley J et al. Case report: hepatolithiasis associated with anomalous biliary anatomy and a vascular compression. HPB Surg. 1991; 3:129.
10. Flecktnstein JF, Frank SM, Thuluvath PJ. Presence of autonomic neuropathy is a poor prognostic indicator in patients with advanced liver disease. Hepatology 1996; 23:471.
11. Health and Policy Committee, American. College of Physiology. How to study the gallbladder. Ann. Intern. Med. 1988; 109:752.
12. Hofmann AF. Bile acid secretion, bile flow and biliary lipid secretion in humans. Hepatology. 1990; 12; 17S
13. Hopman WPM, Jansen JBMJ, Rosenbusch G et al. Role of cholecystokinin and the cholinergic system in intestinal stimulation of gallbladder contraction in man. J. Hepatology. 1990; 11:261.
14. Lundgren O, Svanvik J, Jivegard L. Enteric nervous system ii. Physiology and pathophysiology of the gallbladder. Dig. Dis. Sci. 1989; 34: 284...;
15. Meier PJ. Тhe bile salt secretory polarity of hepatocytes. J. Hepatol. 1989; 9:124.
16. Shiffman ML, Sugtrman HJ, Moore EW. Human gallbladder mucosal function. Gastroenterology 1990; 99:1452.
Treatment
Drug therapy
When prescribing treatment by a gastroenterologist, the following may be used:
- choleretic agents (Gepabene, Flamin, Allochol, Odeston), which help get rid of bile stagnation and avoid stone formation;
- antispasmodics (Drotaverine, Baralgin), which help cope with severe pain;
- antibiotics that help get rid of the inflammatory process.
Surgery
Cholecystectomy is the removal of the gallbladder
Treatment through surgery is prescribed if the outflow of bile is completely blocked, which leads to rupture of the organ. To prevent such a situation, the surgeon completely removes the damaged organ.
The operation is carried out as follows:
- The patient is under general anesthesia.
- An incision in the skin and tissue is made in the navel area, and a cannula is inserted into the incision.
- To inspect the internal cavity, a special instrument attached to the camera is inserted.
- Using fixed cannulas, the gallbladder is separated from the walls and the affected internal organ is removed.
- The incisions made are sutured by the surgeon.
Traditional medicine
Traditional methods of treating the disease are prescribed by a gastroenterologist in combination with medications. They help cope with the symptoms of the disease.
| Collection of choleretic herbs | The medicine is purchased at the pharmacy. It consists of a set of several herbs: chamomile flowers, calendula, yarrow leaves, mint and tansy. To prepare the medicine, 2 tbsp. l. herbs are poured with 1 tbsp. boiled water, the resulting solution is prepared in a water bath for 10-15 minutes. 1 tbsp. The decoction is taken for one month. |
| Corn silk | Dry collection in the amount of 1 tbsp. l. mixed with 1 tbsp. boiled water and leave for 2-3 hours. The decoction is taken three times a day, 50 g each. This decoction helps to cope with bile stagnation. |
| Mint and chamomile | The herbs are mixed in equal proportions and 250 ml is added. boiled water. Insist for one hour. Take 100 ml 3 times a day. |
| Gentian | 1 tbsp. l. 500 ml of dry grass is poured. water, infused for eight hours. Accepted 1 tbsp. before eating. |
It must be remembered that without consulting a doctor, taking the above remedies is not only harmful, but also life-threatening. Only a specialist can prescribe medications to avoid complications and aggravation of the disease.
Diet
You will have to give up flour and sweets
One of the main ways to get rid of the disease is to review your diet and create a special diet. The gallbladder is an organ of the gastrointestinal tract, so it is very important to follow special nutritional rules to get rid of the disease.
When re-tying you should:
- consume low-fat dairy products;
- include stewed, boiled meat and seafood in the diet;
- eat chicken and turkey meat, as it is dietary;
- limit the consumption of vegetable oils;
- eat vegetable dietary soups, fish soup made from lean fish;
- exclude sweet, fatty, smoked foods, salty and peppery foods, carbonated drinks, fast food, spicy foods, canned food;
- eat warm food, avoiding cold and hot;
- eat more fresh vegetables and fruits;
- drink 2 liters of clean drinking water every day, since water is the main assistant in removing toxins and harmful substances from the body;
- Chew food thoroughly.
If you follow a special diet, the symptoms of the disease will quickly go away, and the internal organ will soon return to normal.
Description
The gallbladder is a part of the gastrointestinal tract that is necessary for the secretion of bile. It helps the body in the digestion process. In a healthy body, the shape of the organ is presented in the form of a pear or funnel.
If the deformation of an organ occurs on one side, this is called a bend. Constriction – narrowing along the entire diameter. It does not always negatively affect the body, but only in the following cases:
- violation of the outflow of bile;
- the appearance of inflammation, which is accompanied by a painful syndrome;
- stagnation of bile, leading to changes in metabolism.
Fact! The disease can be detected immediately after the birth of a child, if the cause is an abnormality in the structure of the organ. If a disease is missed, it becomes difficult to differentiate the cause. It is detected during dynamic monitoring of the patient, constant instrumental and laboratory research methods.
Preventing complications
With the help of nutrition, you can prevent some complications and restore impaired functions. If the reason for cholecystectomy was the presence of stones in the bladder, complications such as duodenitis, dyskinesia, cholangitis, and sphincter of Oddi insufficiency may develop.
In order to correct the condition, all foods that contribute to increased bile secretion are removed from the diet:
- any fats, including vegetable fats;
- coarse fiber;
- onion, garlic, radish;
- fatty meat and fish;
- soups with meat, fish and mushrooms.
It is also necessary to reduce or eliminate salt
and
drink less fluid
. Products harmful to the pancreas are excluded - everything that is rich in fiber, contains uric acid and extractives (offal, some types of fish, seafood).
Prevention
The disease can be acquired. To prevent the development of the disease, you should:
- monitor your diet: consume less canned goods, hot dogs, GMO foods, fried, spicy and fatty foods;
- perform daily physical activity with a sedentary lifestyle: walking, light jogging, therapeutic exercises.
At the first signs of illness, you should contact a specialist for advice and a full diagnosis. You should not rely on painkillers, as you need to eliminate the problem, not the symptom.
Prohibited and permitted products after cholecystectomy
There are not many dietary restrictions. they concern food that is not very healthy even for a healthy body.
| Types of products and dishes | Allowed | Prohibited |
| Flour products |
|
|
| Fermented milk | Any with a low fat percentage. |
|
| Meat, offal |
|
|
| Fish | Any cod species. |
|
| First meal |
|
|
| Eggs | Only in the form of omelettes (no more than 2 eggs per week). | Soft-boiled eggs, fresh. |
| Porridge |
| Porridges from any legumes |
| Vegetables |
Very limited - tomatoes and cucumbers. |
|
| Fruits | Any | |
| Fats | Only vegetable ones, preferably olive oil. | Butter. |
| Sausages and fast food products | Only boiled sausages | All smoked meats, any semi-finished products and fast food. |
| Beverages |
|
|
All pickled, salted and canned foods are prohibited. You can only drink homemade compotes prepared for the winter, diluting them with water.
[media=
https://youtu.be/xM9CCaQ9Jqw
]