Metastases are secondary foci in various organs, the result of the spread of a malignant tumor in the body. According to statistics, about 53% of patients with pancreatic cancer already have distant metastases at the time of diagnosis.
- Features of metastasis in pancreatic cancer
- Where do pancreatic malignant tumors most often metastasize?
- What are the dangers of metastases in pancreatic cancer? Possible complications
- Modern diagnostic methods
- Treatment of pancreatic cancer with metastases
- Forecast
It is difficult to fight such an advanced disease. Remission (complete “cleansing” of the body from tumor foci - in a sense, this term can be considered synonymous with recovery) is impossible. But there are treatments that help to slow down the progression of the disease to some extent, cope with painful symptoms and improve the patient's condition.
The goal of treating metastatic pancreatic cancer is to prolong the patient's life and control pain and other symptoms.
Features of metastasis in pancreatic cancer
Considerable progress has been made in the treatment of pancreatic cancer in recent years. However, it is still on the list of cancers with the worst prognosis. The chances of such a patient staying alive for five years are only 9%. At stage IV, when there are distant metastases, the five-year survival rate is 3%.
In general terms, metastasis of any malignant tumor occurs as follows. Some cancer cells break away from the main site and enter the blood or lymphatic vessels. They migrate with the blood or lymph flow, settle in various organs and, under certain circumstances, give rise to secondary foci - metastases.
The mechanisms of metastasis of malignant pancreatic tumors are not yet fully understood. But advances in molecular biology have been able to shed light on some nuances. Disturbances in the functions of certain proteins and genes play a role in the spread of cancer cells throughout the body:
- Cell adhesion molecules : E-cadherin, immunoglobulins, integrin. These proteins are located on the surface of the cell and normally ensure its connection with the extracellular matrix and other molecules.
- Matrix metalloproteinases : these enzymes are located outside cells, their function is to destroy proteins of the extracellular substance. They play an important role in the growth and development of cells, their migration, the formation of new blood vessels, and the inhibition of tumor growth.
- Plasminogen/plasmin systems . Plasmin is an active enzyme that is formed from the proenzyme plasminogen; its main function is the destruction of fibrin clots that make up blood clots.
- KAI1 gene . It prevents metastasis, and in pancreatic cancer its activity may decrease.
Tumor cells in the pancreas produce substances that stimulate angiogenesis , the growth of new blood vessels. This may also contribute to the spread of metastases.
Where do pancreatic malignant tumors most often metastasize?
Pancreatic cancer has a high tendency to metastasize. Even with small, less than 2 cm, malignant tumors, secondary lesions can often be detected. This partly explains why many patients already have metastases at the time of diagnosis.
Most often, secondary lesions are found in the following organs:
- Liver - in almost 80% of cases.
- In 40–50% of cases, carcinomatosis (damage by cancer cells) of the peritoneum develops.
- Lungs - in about 40% of cases.
- Lymph nodes in the abdominal cavity - 20%.
- Bones - 10%.
- Adrenal glands - 5–7%.
- Lymph nodes in the chest - 3%.
In less than 10% of cases, metastases from pancreatic cancer are found elsewhere. They can be found in almost any organ, including the diaphragm, brain, heart, gallbladder, kidneys, small and large intestine, pericardium, ovaries, testicles, stomach, skin, thyroid gland, spleen, uterus, bladder.
Even in cases where pancreatic cancer is operable and seemingly at an early stage, there are often already micrometastases in the abdominal organs and bone marrow. is most prone to hematogenous (through the bloodstream) spread, and to a lesser extent - malignant tumors of the head.
Pancreatic cancer can recur as distant metastases after treatment. For example, according to statistics, in 2/3 of operated patients with stages I and II of a malignant tumor, secondary lesions are subsequently discovered.
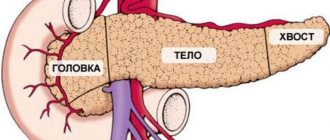
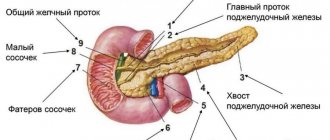
Kinds
According to localization they distinguish:
- tumors of the head of the pancreas, accounting for 50-60% of all cases of the disease;
- tumors of the gland body – up to 10% of cases;
- tail tumors – about 6-8%.
In approximately 25-30% of patients, cancer pathology affects the entire organ.
Based on histological characteristics, they are distinguished:
- adenocarcinomas - neoplasms consisting of mutated glandular cells, occur in 85-95% of patients;
- neuroendocrine tumors;
- cystic tumors of a malignant nature.
What are the dangers of metastases in pancreatic cancer? Possible complications
Metastases are themselves a serious complication of any malignant tumor. They lead to the death of cancer patients in most cases.
Secondary lesions in the liver can lead to disruption of the outflow of bile and the development of jaundice . bilirubin, increases . The skin, mucous membranes and whites of the eyes turn yellow, causing itchy skin. The patient's condition and prognosis worsen, and the possibilities for active antitumor treatment are reduced.
With peritoneal carcinomatosis, the life expectancy of patients is reduced to 4–6 months, and this condition is very difficult to combat.
Ascites , can result from liver damage and peritoneal carcinomatosis . The abdomen increases in size, there is a feeling of heaviness, dull aching pain. When there is a lot of fluid, it restricts the movements of the diaphragm, shortness of breath occurs. Due to compression of the stomach and intestines, nausea, belching, and upset stool are bothersome. Urination is impaired.
Pancreatic cancer with metastases to the lungs can be complicated by exudative pleurisy . In this condition, fluid accumulates between the layers of the pleura , a thin film of connective tissue that lines the inside of the chest cavity and covers the lungs. This condition manifests itself in the form of weakness, shortness of breath, cough, and chest pain. In severe cases, the fluid causes compression of the lung, its ventilation significantly worsens, and blood flow to the heart is disrupted. Pulmonary heart failure develops , which can lead to death.
Bone metastases lead to weakening of bone tissue and pathological fractures from light loads. In more than half of the cases, the femur is affected. Pathological fractures of the vertebrae are especially dangerous, since they cause compression of the spinal cord, and if not treated in time, neurological damage becomes irreversible.
Up to 85% of patients with bone metastases from pancreatic cancer experience excruciating pain in the bones, which intensifies during exercise and at night.
Due to the intense destruction of bone tissue, the level of calcium in the blood increases - hypercalcemia . Its most common symptoms are: nausea, vomiting, abdominal pain, lack of appetite, weakness, lethargy, depression of consciousness, and heart rhythm disturbances. As this complication progresses, the functions of various organs are disrupted, and the patient dies due to cardiac arrhythmia or severe renal dysfunction. Half of patients with hypercalcemia die within a month. Average survival is 10 to 12 weeks.
Symptoms
The initial symptoms of pancreatic cancer are nonspecific and can easily be attributed to poor health, but they should never be neglected. In the early stages the disease manifests itself:
- discomfort in the upper abdomen;
- extreme thirst, frequent urination and other signs of diabetes;
- weakening of stools up to liquefaction, frequent urge to defecate;
- fatigue, decreased performance, loss of appetite.
As the tumor grows and the disease progresses, more serious symptoms develop:
- pain in the upper abdomen, often radiating to the back;
- yellowing of the sclera of the eyes and skin due to disturbances in the outflow of bile;
- nausea, periodic vomiting;
- digestive disorders due to decreased production of digestive enzymes;
- body weight loss.
Modern diagnostic methods
If pancreatic cancer is suspected, the doctor will most likely order a CT scan first. The images clearly show the pancreas; you can detect not only the primary tumor, but also its spread to neighboring organs and distant metastases. In addition, CT allows one to evaluate the possibility of surgical treatment.
The most informative is multi-slice computed tomography (MSCT) with multiphase intravenous bolus contrast . During this study, images are taken at certain intervals after intravenous administration of contrast solutions.
The diagnosis is usually confirmed with a biopsy. The doctor obtains a certain amount of pathologically altered tissue from the pancreas and sends it to the laboratory for cytological and histological examination. This can be done using a needle inserted through the skin under CT scan guidance.
Magnetic resonance imaging
Sometimes MRI is used to diagnose pancreatic cancer and its metastases. In some cases, special techniques are used:
- MR cholangiopancreatography - study of the condition of the bile ducts and pancreatic duct.
- MR angiography is the study of blood vessels.
Ultrasonography
When a patient is bothered by incomprehensible abdominal symptoms, most often an examination is prescribed with an ultrasound. But computed tomography is much more informative in diagnosing pancreatic cancer and its metastases.
Valuable data can be obtained using endoscopic ultrasound - endosonography , or endosonography . A miniature ultrasound sensor is used at the end of an endoscope, which the doctor inserts into the stomach and duodenum. A needle can also be inserted through an endoscope to perform a biopsy. Such a study is available in the European clinic.
Cholangiopancreatography
This study is used to check whether a pancreatic tumor or its metastases has blocked the bile ducts. The procedure can be performed in two ways:
- Retrograde cholangiopancreatography (RCPG) . This is an endoscopic procedure. The doctor inserts an endoscope into the duodenum, inserts a thin catheter into the bile ducts and fills them with a radiopaque solution. After this, the areas of narrowing are clearly visible on radiographs. During ERCP, you can install a drainage tube, perform a biopsy, and install a stent - a tube with a mesh metal wall that will expand the lumen of the blocked section of the duct and ensure normal outflow of bile.
- Percutaneous transhepatic cholangiography is performed with a needle through the skin. Typically, this method is used when, for various reasons, it is not possible to perform RCCP.
PET scan
Positron emission tomography is the gold standard for detecting distant metastases in modern oncology. The essence of the procedure is that a weak radioactive drug is injected into the patient’s body, which actively accumulates in tumor cells. Then the images are taken using a special device. All secondary tumor foci are clearly visible on them.
PET is even more informative if combined with computed tomography. With the help of CT, a high-quality image of different areas of the body is created, and with the help of PET, areas in which the radioactive drug accumulates are superimposed on it.
Laboratory research
For jaundice, a biochemical blood test is prescribed: the levels of different fractions of bilirubin and other substances that are markers of liver function are determined. A blood test helps assess the degree of deterioration of the organ and distinguish obstructive jaundice associated with impaired bile outflow from parenchymal jaundice caused by the destruction of liver cells - hepatocytes.
Metastases in the lungs - symptoms
With single foci, the disease is often asymptomatic. As the disease progresses, the following signs appear:
- shortness of breath, chest pain, difficulty breathing;
- cough - dry or with sputum;
- hemoptysis.
Since metastasis indicates that the primary tumor has grown to the third or fourth stage, its symptoms can manifest themselves quite noticeably: digestive problems, ascites, bleeding, etc. Also, most patients experience conditions common to different types of oncology, such as:
Our expert in this field:
Ivanov Anton Alexandrovich
Medical director, oncologist-surgeon, candidate of medical
sciences Call the doctor
Call the doctor
- weakness, anemia, increased fatigue;
- loss of appetite, sudden loss of body weight;
- low-grade fever (37–38 ⁰С), which does not decrease when taking antibiotics or antipyretics;
- pain syndrome.
For diagnosis, ultrasound, fluorography, MRI, CT or PET, histological studies and other methods are used.
Treatment of pancreatic cancer with metastases
For pancreatic cancer with metastases, surgical treatment is not used. The main way to fight a malignant tumor is chemotherapy. The choice of treatment tactics largely depends on the general condition of the patient and the morphological affiliation of the tumor. If it is bad, only one chemotherapy drug is prescribed, usually gemcitabine or capecitabine.
If the patient is in good condition, it is preferable to use the FOLFIRINOX combination of chemotherapy drugs. This regimen includes four drugs: 5-fluorouracil, irinotecan (Camptosar), leucovorin, oxaliplatin (Eloxatin).
If BRCA1, BRCA2, or PALB2 mutations are found in tumor cells, a combination of gemcitabine and cisplatin or olaparib (Lynparza) may be considered as treatment options. The latter is a targeted drug; it blocks the enzymes poly(ADP-ribose) polymerase (PARP).
The choice of chemotherapy agents for stage IV pancreatic cancer is limited, so patients whose condition allows them to tolerate active treatment should consider participating in clinical trials.
If first-line medications no longer help, your doctor may prescribe second-line treatment. Some possible schemes:
- FOLFIRI: 5-fluorouracil + leucovorin + irinotecan.
- OFF, FOLFOX: oxaliplatin + 5-fluorouracil + leucovorin.
- Capecitabine + oxaliplatin.
In some cases, radiation therapy is used to control symptoms.
Sometimes patients with stage IV pancreatic cancer benefit from pembrolizumab (Keytruda), an immunodrug from the group of checkpoint inhibitors. It blocks PD-1, a molecule that is found on the surface of immune cells and, by binding to PD-L1, a protein that can be found on the surface of cancer or other cells, suppresses the antitumor immune response.
Pembrolizumab activates the immune system, causing it to recognize and attack a malignant tumor. In 2021, the US Food and Drug Administration (FDA) granted accelerated approval to the targeted drug larotrectinib (Vitraqui). It is effective against various types of malignant tumors, including the pancreas, if the cancer cells have certain mutations.
It is possible to use chemoradiotherapy - a combination of chemotherapy drugs with irradiation of tumor foci. This treatment may be more effective, but it carries a higher risk of serious side effects.
Treatment of complications of pancreatic cancer metastases:
With obstructive jaundice, the outflow of bile can be restored using external, internal or external-internal drainage. During ERCP or percutaneous transhepatic cholangiography, a drainage tube is installed in the bile ducts, which drains bile out into the lumen of the duodenum or in both directions. A more modern solution is stenting, when a stent is placed in the blocked area during ERCP. It is a tube with a mesh wall made of metal or polymer.
For peritoneal carcinomatosis, in some cases, the modern technique of hyperthermic intraperitoneal chemotherapy (HIPEC) . If the cancer is confined to the abdomen, the surgeon may remove any large tumor lesions and then flush the abdomen with a warmed chemotherapy solution to destroy any remaining cancer cells. Unfortunately, HIPEC is not suitable for all patients. In order for such treatment to be carried out, there must be no metastases outside the abdominal cavity, all large lesions must be resectable, and the patient must be in a state of health that allows major surgery.
For chronic pain, medications are prescribed in accordance with the “pain ladder” recommended by the World Health Association. Nerve blocks are indicated for some patients with metastatic pancreatic cancer.
For ascites, laparocentesis is indicated - a procedure during which a puncture is made in the abdominal wall to remove fluid. Peritoneal catheters are installed to ensure constant fluid drainage . Some patients require surgery to prevent fluid accumulation.
For exudative pleurisy, thoracentesis is indicated - a procedure in which fluid is removed from the pleural cavity through a puncture. Systemic chemotherapy helps prevent its further accumulation. If it is ineffective, pleurodesis is performed - a procedure during which a drug is injected between the layers of the pleura, as a result of which they stick together and fluid stops accumulating between them.
For bone metastases, drugs from the bisphosphonate group are used to prevent bone loss. If there is a high risk of pathological fracture, the bone can be strengthened with metal plates or screws. With their help, you can restore the integrity of the bone if a fracture has already occurred. In some cases, special bone cement is used.
Forecast
To assess prognosis in oncology, the five-year survival rate is used - the percentage of patients who remain alive within five years from the date of diagnosis. For pancreatic cancer with metastases, this figure is about 3%. This is the worst prognosis among all tumors of the digestive system.
But even such a terrible diagnosis is not a reason to give up. There are effective treatments that help prolong the patient's life. Literally every year the possibilities of oncology are growing. Even if the patient managed to give an extra week of life without pain and other painful symptoms, it was worth fighting for. For us there are no hopeless patients. Contact us to find out more about treatment options at the European Clinic.
Book a consultation 24 hours a day
+7+7+78
Rehabilitation
Recovery after surgery is an important stage in the treatment of pancreatic cancer, including:
- analgesic therapy, elimination of painful curvatures of the body;
- expansion of bile ducts narrowed after surgery, treatment of inflammation;
- careful care of surgical sutures;
- a gentle diet;
- regular administration of insulin, other hormones and enzymes;
- physiotherapeutic procedures, etc.
Hormone and enzyme replacement therapy after radical surgery is necessary for the patient for the rest of his life.