Gastric cancer (GC) remains one of the most common causes of death from malignant tumors worldwide [1, 2]. Determining the factors influencing the prognosis of GC is important both for diagnosis and for the search for new treatment regimens for this disease. One of these factors is the severity of inflammatory changes in the tumor and adjacent tissues. However, the assessment of its role in tumor progression is ambiguous. Some authors believe that high infiltration of the tumor and adjacent tissues by immune cells may be associated with antitumor activity and better survival of cancer patients [3, 4]. Others have suggested that tumor-associated lymphocytes and macrophages may be associated with tumor progression [5–8]. It should be noted that most studies are related to the study of the role of T-lymphocytes and macrophages in tumor progression [3, 8, 9], while the role of B-lymphocytes remains practically unexplored. In this regard, the purpose of this study was to study the characteristics of peritumoral infiltration of the gastric mucosa (GM) by B lymphocytes and their relationship with the clinical characteristics of gastric cancer.
Epidemiology
The pathology is not associated with age, although it is more often detected in older people and children in the first year of life.
By gender – it mainly occurs in women.
The prevalence of lymphofollicular gastritis ranges from 2 to 4% among all chronic forms.
A distinctive feature is the presence of diffuse lesions in 2/3 of patients: in 15-18% of patients the fundic form of lymphocytic gastritis is detected, and in 6-8% - the antral form.
All variants of this type of pathology require complex treatment.
Erosive and hemorrhagic gastritis
Clinical signs.
Lesions in hemorrhagic and erosive gastritis are most often detected in seriously ill patients (stress lesions), in patients taking nonsteroidal anti-inflammatory drugs (NSAIDs), in heavy drinkers, and as a result of limited gastric trauma with a nasogastric tube or vomiting. In the case of seriously ill patients and patients taking NSAIDs, its prevalence is more than 50%. Erosions and hemorrhages are grouped together because both types of damage are commonly found in these conditions. Mucosal ischemia and prostaglandin inhibition are important mechanisms in the development of these lesions. Erosions and hemorrhages in the stomach do not always cause abdominal pain syndrome, and even when it is present, as in the case of patients taking NSAIDs, the correlation between its intensity and the number of erosions is weak. Erosions and hemorrhages are rarely the causes of significant gastrointestinal bleeding. Consequently, erosions and hemorrhages are more impressive during endoscopy than clinically.
Endoscopy and biopsy.
The literal definition of erosion is partial destruction of the mucosa, which does not extend below the muscular plate of the mucosa to another layer of the intestinal wall - the submucosal layer. Ulcers, on the other hand, are mucosal damage that extends beyond the mucous membrane into the submucosal layer. At endoscopy, differentiation between erosion and ulceration is arbitrary, especially with large (greater than 5 mm) lesions that appear shallow. Lesions are usually described as erosions if they are small and their base is not deepened or the deepening is minimal. A typical erosion has a white base surrounded by a halo of erythema. These aphthae-like lesions are often multiple. Submucosal hemorrhages appear as scattered petechiae or bright red spots that look like “blood under plastic wrap.” In clinical practice, erosions and hemorrhages are diagnosed based on the endoscopic picture and a biopsy is not usually taken. The exception is in patients with compromised immune systems, where a biopsy should be taken to exclude opportunistic infections, especially cytomegalovirus. The mucosa immediately adjacent to erosions and ulcers often exhibits severe epithelial damage with minimal inflammation. As stated earlier, this should be referred to as reactive gastropathy. At a clinical level, if a patient has been taking an NSAID, for example, they may be diagnosed with NSAID-associated gastropathy. In patients with subepithelial hemorrhages, the term hemorrhagic gastropathy replaces the term hemorrhagic gastritis because inflammatory cell infiltration is often minor, whereas vascular changes are the most characteristic feature.
Etiology and pathogenesis
The causes of the disease are not completely clear.
Reasons for development
In the etiology of lymphocytic gastritis, researchers have proposed 2 main versions:
- Link to gluten intolerance.
With celiac disease, an immune response develops to the penetration of gluten protein (a protein from grain crops) into the body. Immune cells - lymphocytes - infiltrate the mucous membrane to protect the surface of the stomach from foreign protein. Lymphocytic infiltration in celiac disease is usually detected in the small intestine. But, according to the latest information, 15-20% of children with gluten enteropathy simultaneously develop lymphoid lesions of the stomach.
- Association with Helicobacter pylori infestation.
Numerous studies have shown that Helicobacter pylori infection causes an immune response - infiltration of the stomach with lymphocytes and the production of antibodies to Helicobacter pylori.
Important! Patients infected with Helicobacter pylori and patients with gluten intolerance are at risk for developing lymphocytic gastritis.
Development mechanisms
The development of lymphoid gastritis is based on an unusual reaction of the immune system to external stimuli.
In the case of celiac enteropathy, the body perceives the gluten protein as an antigen, which causes the accumulation of lymphocytes in the stomach, ready to fight gluten.
With Helicobacter pylori etiology:
- The bacteria attach to the lining of the stomach.
- They alkalize the environment around them with waste products, creating a “lifeline.”
- They grow in numbers, forming colonies.
- They actively damage the epithelium of the mucosa and cause chronic inflammation in the wall of the stomach, which is accompanied by autoimmune reactions with a characteristic accumulation of lymphocytes in the intercellular space of the mucous membrane.
Against this background, in addition to damage to the stomach, the development of duodenitis, inflammation of the duodenum, is possible.
results
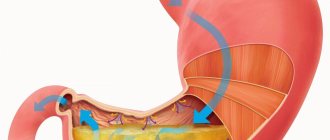
The study of the characteristics of the expression of CD20 B-lymphocytes made it possible to identify three types of structures associated with this marker: individual B-lymphocytes located diffusely, LF and focal lymphoid infiltrates (LI). Diffusely located B lymphocytes were of two types. The first type was represented by round-shaped cells with clear, even contours and a thin rim of cytoplasm (see figure a, and below). The second was cells of irregular shape with unclear contours, having a large number of cytoplasmic processes, as a result of which the expression of the marker in them seemed fragmented (see figure, b). Ochagovye L.I. bordered directly on the invasive edge of the tumor (see figure, c) and consisted predominantly of cells of the second type. LFs were located predominantly in the coolant adjacent to the tumor. LFs without light centers, with light centers, and LFs with atypical light centers were noted (see figure, d). Unlike ordinary light centers, atypical light centers were irregular in shape, often located along the periphery of the follicle, and the cells that formed them did not express CD20.
Rice. 1. Features of the expression of CD20 B lymphocytes in the peritumoral region of the gastric mucosa. a — expression of CD20 in round-shaped cells, with clear, even contours and a thin rim of cytoplasm, ×400; b — expression of CD20 in cells of irregular shape, with unclear contours, having a large number of cytoplasmic processes, ×400; c — focal lymphoid infiltrates (li) bordering the invasive edge of the tumor (arrows), ×100; d — lymphoid follicles in the gastric mucosa adjacent to the tumor. sc – light centers, asc – atypical light centers, ×100. Immunohistochemical staining with antibodies to CD20.
The density of diffuse CD20 B lymphocytes depending on the clinical characteristics of GC is presented in the table. The lowest density values were observed in poorly differentiated adenocarcinoma and undifferentiated GC (G3-G4), with tumor invasion depth T1-2 and in the presence of metastases in regional lymph nodes (N1-2). There were also positive correlations between the density of diffuse CD20 B lymphocytes in the tumor and the presence of focal LI ( ρ
=0.634,
t
=3.28,
p
=0.005).
The density of diffuse CD20 B lymphocytes was higher in the presence of LI than in the absence (49.0 ± 15.4 and 22.9 ± 12.1 cells per UEP, respectively, p
= 0.009). No connection was found between this indicator and the survival of patients with cancer and with the location of the tumor and type of growth.
Density of CD20 B lymphocytes in the gastric mucosa and tumor stroma depending on the clinical and morphological characteristics of gastric cancer Note.
* — differences when comparing G3-G4 and RCC; ** - when comparing T1-2 and T3-4 in the tumor; *** - when comparing N0 and N1 in the coolant; **** - when comparing N0 and N2 in the coolant. The presence of focal LI was negatively correlated with the histological type (gamma = –0.524, Z = –2.02, p
=0.04) and overall 3-year survival (gamma =–0.770, Z=–2.60,
p
=0.01).
Ochagovye L.I. were more often observed in the diffuse type of gastric cancer than in the intestinal type (in 46.7 and 21.4% of cases, respectively, p
= 0.15).
Despite the fact that no connection was found between this indicator and the depth of tumor invasion and the presence of metastases in regional lymph nodes, the presence of focal CD20 LI was accompanied by a statistically insignificant decrease in 3-year overall survival from 94.7 to 70.0% ( p
= 0.07) . However, there was no connection between focal LI and 3-year relapse-free survival of GC patients.
Similarly, the amount of LF in the GM adjacent to the tumor correlated with the histological type (gamma = 0.509, Z = 2.39, p
=0.02) and 3-year disease-free survival (gamma =–0.636, Z=–2.51,
p
=0.01).
Multiple L.F. were more common in the diffuse type of GC than in the intestinal type (in 72.7 and 38.9%, respectively, p
= 0.07), and in their presence, a decrease in 3-year relapse-free survival was noted from 75 to 40%,
p
= 0, 08). At the same time, no connection was found between this indicator and 3-year overall survival.
The presence of LF with atypical light centers correlated only with the severity of gastric dysplasia (gamma = 0.833, Z = 3.22, p
=0.001).
Most often they were detected in cases of severe dysplasia of the gastric epithelium (in 50.0 and 12.5%, respectively, in the presence or absence and severe or moderate degree of dysplasia of the gastric epithelium, p
= 0.02).
Clinical manifestations of chronic gastritis
Symptoms of lymphoid gastritis are nonspecific and often depend on the level of acidity of gastric juice.
- Constipation
- Heartburn
- Low pressure
- Sweating
- Nausea
- Feeling of heaviness
Symptoms of the disease
Manifestations of increased secretion of gastric juice in many studies were observed in a group of patients with Helicobacter pylori infection; low acidity was not associated with HP.
| Symptom | Increased secretion (usually associated with Helicobacter pylori) | Decreased secretion |
| Localization of pain | In the epigastrium, right hypochondrium | |
| Nature of pain | Strong, cramping | Spilled character |
| Time of onset of pain | On an empty stomach, 1.5-2 hours after eating; subside after eating | Immediately after eating |
| Chair | Tendency to constipation | Stool disorder – tendency to liquefy. Bloating, rumbling |
| Belching | Acidic air, heartburn | Rotten air |
| Saturation | Quick satiety with the usual amount of food, feeling of heaviness and fullness in the stomach | |
| Additional signs | Nausea, tendency to bradycardia, sweating, low blood pressure | Bloating, rumbling after eating, nausea |
During the examination, the doctor identifies the following signs in the patient:
- the tongue is covered with a white or yellowish coating;
- pain in the epigastric and pyloroduodenal zone upon palpation;
- weight loss;
- pallor;
- brittle hair and nails are signs of polyhypovitaminosis that appear over a long period of time.
The peculiarities of the clinic allow the doctor to clarify the nature of changes in gastritis and identify the presence of symptoms of damage to the liver and pancreas.
Diagnosis of the disease
Treatment of lymphocytic gastritis is carried out taking into account the results of a comprehensive examination of the patient.
Primary diagnosis of pathology
The diagnosis is based on the collection of complaints, clarification of the medical history and an objective examination of the patient.
Laboratory diagnosis using conventional methods for lymphoid gastritis is uninformative and not specific.
It is advisable to conduct the examination using different methods:
- A general blood test is unremarkable or reveals signs of anemia.
- Blood biochemistry – monitoring of liver and pancreas disorders.
- Coprogram – assessment of digestive function, inflammatory changes.
- Gregersen's reaction - detection of blood in the stool (positive in the presence of erosions, bleeding).
- Urease test for Helicobacter Pylori (Hp) is positive for Helicobacter pylori infection.
- Determination of acidity (gastropanel).
- Detection of antibodies to the protein gliadin (in combination with celiac disease).
Especially important for choosing treatment tactics for gastritis are the Gregersen reaction, methods for detecting HP and determining acidity.
A decrease in hemoglobin in a general blood test is a reason to clarify the cause of anemia.
Vitamin B12 deficiency in blood serum is associated with malnutrition (strict vegetarian diet, psychological factor of malnutrition), decreased synthesis of intrinsic Castle factor in atrophic gastritis.
Lack of serum iron, transferrin, and a decrease in the total iron-binding capacity of blood serum are detected when iron absorption is impaired as a result of decreased secretion of gastric juice and hydrochloric acid in hypoacid gastritis.
In-depth diagnostics
To make a diagnosis if gastritis is suspected, it is important to conduct studies that provide reliable information about the condition of the gastric mucosa: the nature, location and severity of changes. Instrumental methods help to diagnose lymphocytic gastritis:
- gastroscopy with targeted biopsy and collection of at least 5 biopsy specimens - assesses the localization of lesions in the gastric mucosa (GM) - total lesions, lesions in the area where the stomach enters the intestines, lesions in the fundus of the stomach; the presence of erosions, uniformity of inflammation (the most pronounced hyperemia and swelling of the epithelial layer are observed at the site of Helicobacter colonization); symptoms of atrophy of the gastric mucosa;
- Helpil test system - express diagnosis of helicobacteriosis by the urease activity of a biopsy sample, a biopsy sample of the mucous membrane is placed on the test system disk, staining the disk blue for 3 minutes confirms the presence of Helicobacter pylori;
- gastropanel - a serological method for determining antibodies to Helicobacter pylori in venous blood; determination of the concentration of hormones produced by the gastric glands - gastrin, pepsinogen 1,2 - is used to diagnose atrophy of the gastric mucosa;
- Ultrasound of the abdominal organs - reveals signs of damage to the liver, pancreas, bile ducts, often combined with gastritis.
Note! Endoscopic and histological methods clarify the degree of inflammation of the stomach, the area of distribution, the type of gastritis and are the most important.
Structural features of tissue damage in lymphocytic gastritis
Modern equipment of clinics makes it possible to examine the patient in detail and identify lesions of the gastrointestinal tract characteristic of a specific pathology. This helps to build adequate treatment regimens, which significantly improves the prognosis.
An endoscopic examination reveals:
- swelling, spotty or diffuse hyperemia of the mucous membrane;
- granular accumulations of lymphocytes in the form of papillae, nodules in the interepithelial space of the stomach;
- numerous erosions due to inflammation.
Histological examination of the biopsy specimen determines the nature and extent of tissue damage to the gastric wall, cell changes, and signs of foreignness, which are important for assessing the possibility of cancer risk. In addition, gastroscopy with targeted biopsy reveals the presence of Helicobacter pylori colonies.
Causes of infiltration of the mucous membrane by lymphocytes
The reason for the migration of immune cells into the epithelial layer of the gastric mucosa is the reaction of the immune system: while the action of the irritating agent (gluten, Helicobacter) persists, infiltration by lymphocytes leads to excessive growth of the mucosa and triggers autoimmune processes.
Discussion
The role of tumor-infiltrating immune cells in the progression of malignant tumors has been confirmed in a large number of studies. It is believed that the main mechanisms may be associated with the secretion of cytokines, chemokines, growth factors and proteases by immune cells [6, 7, 10], activation of angiogenesis [4, 5, 11], with the participation of immune cells in the remodulation of the extracellular matrix, promoting tumor invasion cells and metastasis to distant organs [4, 6]. The role of B lymphocytes in tumor progression remains poorly understood. Our results indicate the heterogeneity of CD20-expressing structures in the peritumoral region of the gastric mucosa. They were represented by diffuse B-lymphocytes, LF and focal LI. It is interesting that a high density of diffuse B-lymphocytes was statistically significantly associated with the initial stages of the disease and was not associated with long-term results of treatment for cancer, while the presence of focal LI and multiple LF was associated with the diffuse type of cancer and worsening long-term results of treatment for this pathology.
Literature data are scarce and ambiguous. A number of authors indicate that an increase in the number of B lymphocytes is a prognostically favorable sign, as it is associated with specific antitumor immunity [12, 13]. However, other researchers have noted that B lymphocytes may contribute to the progression of malignancies. Thus, it was shown that in tumor-infiltrating B lymphocytes there is activation of “signaling protein and activator of transcription 3” (STAT3). STAT3 is known to play an important role in tumor angiogenesis, participating in the regulation of the expression of vascular endothelial growth factor (VEGF) and other pro-angiogenic factors [14, 15]. The density of tumor-infiltrating B cells has been shown to directly correlate with the expression levels of VEGF, matrix metalloproteinase 9 (MMP9), and hypoxia-inducible factor 1a (HIF1a) [16, 17]. An increase in the level of B lymphocytes with activated STAT3 was noted in gastric, lung, liver, and prostate cancer and was associated with worse long-term treatment outcomes [16]. In addition, it has been shown that B lymphocytes themselves can be a source of VEGF-A, which plays a key role in lymphogenesis and angiogenesis [18], and B lymphocytes expressing interleukin 10 can contribute to the polarization of M1 macrophages, which have antitumor activity, in M2, macrophages have the ability to stimulate the growth and metastasis of malignant tumors [19, 20].
Differential diagnosis
Differential diagnosis is carried out with other types of gastritis.
| Type of gastritis | Lymphocyte gastritis | Eosinophilic gastritis | Autoimmune gastritis | Tuberculosis, Crohn's disease, sarcoidosis |
| Features of the anamnesis | No | Characteristic connection with allergies | No | Indication of tuberculosis, heredity |
| Localization of the lesion | Fundus, body, pangastritis (total damage to the mucous membrane of the entire gastric cavity) | Antrum | Fundus and body of the stomach | Antrum, intestines |
| Signs of other diseases | Without features | Rash | Concomitant hormonal pathologies: diabetes mellitus, autoimmune thyroiditis | Enlarged lymph nodes, multiple organ damage in sarcoidosis |
| Endoscopy | Swelling, granularity of the mucous membrane, erosion | Swelling, vulnerability of the mucous membrane | Atrophy of mucosal cells | Swelling, erosion of the intestinal wall |
| Histology | Lymphocyte infiltration | Clusters of eosinophils | Atrophy of the gastric glands | Clusters of lymphocytes, ulcers, granulomatous gastritis |
| Secretion | Can be increased or decreased | Can be increased or decreased | Sharply reduced | Can be increased or decreased |
| Additional laboratory signs | Possible anemia | Eosinophilia | B12 deficiency anemia | Increased fecal calprotectin |
As can be seen from the table, lymphocytic gastritis has many common symptoms with other types of this pathology. An accurate diagnosis is made only after gastroscopy with targeted biopsy.
Examples of diagnosis formulation
The diagnosis of chronic gastritis takes into account the type of this pathology, localization, connection with Helicobacter pylori, endoscopic characteristics, the level of acidity of gastric juice (increased - hyperacid gastritis, decreased - hypoacid gastritis).
Examples of formulation of diagnoses:
- Chronic antral gastritis associated with HP, degree of activity 2, in the acute phase.
- Chronic gastritis associated with HP, atrophic, hypoacid, in the acute phase.
Damage to the transitional region between the stomach and intestines - antral gastritis - is often combined with inflammation of the mucous membrane of the duodenum - in this case the diagnosis sounds like gastroduodenitis. Atrophic changes indicate a long course of the disease, which is also reflected in the formulation of the diagnosis.
A positive result for Helicobacter pylori is an indication for antibiotic therapy. Hypersecretion of hydrochloric acid during gastritis increases the risk of ulcerative lesions. With reduced secretion of gastric juice, there is a high risk of cancer.
Approximate interpretation of a detailed diagnosis:
- Chronic is a sign of long-term inflammation of the stomach.
- The prevalence of the inflammatory process is antral, fundic (bottom of the stomach), diffuse (widespread or total damage to the mucous membrane without specific foci).
- The morphology of the inflammatory process is superficial (damage to the gastric mucosa), erosive (with the presence of erosions of the epithelial layer), hemorrhagic (the presence of hemorrhages on the gastric mucosa), atrophic (atrophy of the gastric glands with decreased secretion of gastric juice, pale, thinned mucosa).
- Inflammatory activity - there are 3 degrees: minimal (1), moderate (2), severe (3); the higher the degree of inflammation, the greater the atrophy of the gastric glands, the higher the risk of tumor damage.
- Contamination with Helicobacter pylori – Hp(+) or Hp(-) – the presence or absence of Helicobacter pylori infection and the need for its treatment.
- The state of the acid-forming function of the stomach is intact, the acid-forming function is reduced (hypoacid), the acid-forming function is increased (hyperacid).
- The period of the disease is exacerbation (active therapy, reduction of inflammation), remission (anti-relapse therapy).
Take note! A detailed diagnosis gives an idea of the duration, prevalence, morphology and depth of the inflammatory process, the need for eradication (destruction) of Helicobacter pylori infection, and determines the tactics of dispensary observation.
Dispensary observation tactics depend on the diagnosis:
- Chronic gastritis - systematic observation, anti-relapse treatment.
- Lymphocytic gastritis - the patient is at risk for the development of oncology and autoimmune lesions of the stomach (at initial registration, annual gastroscopy with biopsy).
- Atrophic gastritis with metaplasia - gastritis with signs of cell degeneration (risk group for oncology), gastroscopy with biopsy 2 times a year.
- Gastritis with increased acid-forming function (risk group for developing peptic ulcers) - anti-relapse therapy in spring/autumn to normalize acid-forming function and prevent ulcer formation.
- HP(+) – if the result is repeated positive, antibiotic therapy.
Topography of gastritis
There are three histological zones in the stomach, the difference of which is based on the type of glands: cardiac, acid-producing (fundic) and antral.
The mucosa at the border of these zones may contain a mixture of two adjacent types of mucosa for several centimeters. The topographic distribution of gastritis is often related to the type of glands. Cardia.
The mucous membrane of the cardia occupies only a few centimeters below the gastroesophageal junction.
Its glands are mainly mucous, similar to the antrum glands. Inflammation of the cardia region (“carditis”) was largely ignored until recently; scientific interest in this area has now arisen. One reason for this is the dramatic increase in cardia cancer in Western countries and the possibility that cardia cancer may develop from intestinal metaplasia at the junction of squamous and columnar epithelium. It is possible that this intestinal metaplasia is a consequence of gastroesophageal reflux disease in some patients. A second reason for interest in "carditis
" is that biopsy in this area may be more sensitive than squamous epithelial biopsy in diagnosing patients with atypical symptoms of gastroesophageal reflux disease.
Acid-producing department.
The acid-producing mucosa occupies the fundus and body of the stomach (the upper three-quarters of the stomach). Acid-producing glands consist of parietal cells that produce acid and intrinsic factor and chief cells that secrete pepsinogen.
Antral region.
The antral mucosa occupies the distal quarter of the stomach and is limited by the angle of the stomach proximally and the pylorus distally. It contains mucous cells and gastrin-producing cells.
Risk factors
In order for a disease to arise and develop, in addition to direct causes, it is important to have conditions conducive to damage to the body.
They are called risk factors and in lymphoid gastritis are often external, controllable.
These include:
- consumption of stale food;
- snacks in fast food establishments, dry food;
- non-compliance with the diet - a break between meals of up to 10-12 hours or more, a late and heavy dinner (often before bedtime);
- poor chewing of food (for dental problems);
- abuse of spicy, smoked, pickled, sweet foods and spices, as well as too cold or too hot food, Coca-Cola and other carbonated drinks;
- stress;
- bad habits (smoking, alcoholism);
- failure to comply with hygiene rules (personal - hand washing, general - washing vegetables, fruits, other foods, dishes, etc.) contributes to Helicobacter pylori infection;
- consumption of products containing cereals (bread, cereal porridge, kvass, etc.) with gluten intolerance.
It is important! Most risk factors contributing to the development of lymphoid gastritis can be excluded independently. If you have concomitant diseases, always follow the recommendations of your doctor.
Treatment methods for lymphocytic gastritis
Treatment of lymphocytic gastritis should be comprehensive - eliminate pain, nausea, and normalize the secretion of gastric juice.
Non-drug therapy
Non-drug therapy:
- giving up bad habits - smoking, drinking alcohol;
- diet therapy;
- herbal medicine with decoctions and complex herbs;
- physiotherapy.
Diet therapy is the main condition for the success of drug treatment, shortens its duration, and increases the period of remission.
Diet for lymphocytic gastritis
Therapeutic nutrition should be frequent, divided: 5-6 times a day.
Principles of dietary nutrition
To properly organize diet therapy, you need to follow the basic principles of food intake for chronic diseases of the gastrointestinal tract:
- Mechanical sparing - exclusion of foods rich in coarse fiber: radishes, beets, carrots, radishes, beans, whole grain bread, nuts, fresh fruits and berries; foods rich in connective tissue: meat with tendons, fish and poultry skin.
- Chemical sparing is the exclusion of irritating foods from the diet: strong meat and fish broths, marinades, canned foods, smoked meats, herbs, spices.
- Physical sparing - temperature regime of dishes from 15 to 60 °C (maximum gentle temperature - 37 °C), reheating is unacceptable.
- Reducing the daily amount of food to 2-2.5 kg.
- Recommended food processing methods: steaming, boiling, stewing.
- Consistency: during an exacerbation - semi-liquid, mushy food, after the pain disappears, switch to food in small pieces.
The result of treatment largely depends on compliance with the diet.
Allowed foods for gastritis
Diet for lymphocytic gastritis in the acute period:
- slimy cereal soups with vegetable broth (oatmeal);
- liquid semi-viscous, well-cooked or mashed porridge;
- lean pureed meat or fish in the form of soufflés, quenelles, meatballs made from meat minced twice;
- baked dishes without crust;
- puree from boiled vegetables (zucchini, potatoes);
- low amount of salt.
Note! After an exacerbation, the diet depends on the acidity: when it is low, foods that moderately stimulate the secretion of gastric juice are allowed (milk, fermented milk products, stewed vegetables, vegetarian soups); at elevated levels, milk porridge, pureed cottage cheese, vegetable purees, lean meat in the form of cutlets, jelly, jelly, and a small amount of butter and vegetable oil are allowed.
Prohibited Products
Prohibited on the menu:
- waterfowl meat (refractory fats);
- peas;
- dairy dishes;
- garlic, onion, sorrel;
- mushrooms;
- whole grain bread, muffins, fresh bread, puff pastry;
- pork and lamb fats;
- beets, radishes, radishes;
- boiled and smoked sausages;
- canned food, preserves;
- pastry creams;
- strong meat and fish broths;
- carbonated drinks, coffee.
Forbidden foods can be replaced with dietary options without compromising your taste or health.
General Diet Recommendations
General recommendations characterize the lifestyle of a patient with chronic gastritis:
- Elimination of bad habits (smoking, alcohol).
- Thorough heat treatment and chewing of food.
- Maintaining a meal schedule (on holidays, weekends, on the road).
- Use only fresh, high-quality products for cooking.
- Eating in a calm environment, not “on the run” - setting aside time for eating at least 30 minutes, no later than 3 hours before bedtime.
- Stick to a diet throughout your life.
These rules must be followed constantly, which will prevent exacerbations and complications of lymphoid gastritis.
Traditional methods of treatment
Treatment of lymphoid gastritis also includes herbal medicine. Herbal infusions have a complex effect (soothing, hemostatic, astringent, carminative, anti-inflammatory, regenerating, enveloping, tonic, bactericidal).
For example:
Gastric collection No. 1:
- immortelle, chamomile, calendula – healing of erosions of the gastric mucosa;
- St. John's wort and plantain - anti-inflammatory effect;
- stinging nettle – stopping bleeding from eroded areas;
- corn silk - normalizes the flow of bile, improves digestion;
- dill – eliminates bloating.
Contraindicated during pregnancy and breastfeeding. 1 filter bag is brewed with 200 ml of boiling water, left for 20 minutes and taken half a glass 2 times a day during or after meals, course duration - up to 1 month.
Gastric collection No. 2:
- peony, valerian, motherwort – sedative effect;
- flax seeds – enveloping effect;
- black currant leaf - normalization of acidity;
- Licorice root – anti-inflammatory, antispasmodic effect.
It is used for signs of high acidity, eliminates spasms, pain, heals ulcers and erosions of the digestive tract. 2 filter bags are infused for 30 minutes, take ½ cup in the morning and evening, course duration is 2-3 weeks.
Gastric collection No. 3:
- calamus rhizomes - increased appetite;
- valerian rhizomes – calming and antispasmodic effect;
- buckthorn bark – laxative effect;
- peppermint – choleretic effect, normalization of motility of the digestive tract;
- Stinging nettle improves the flow of bile and reduces flatulence.
Prepared in a water bath (1 tablespoon per 200 ml of boiling water), take half a glass (100 ml) twice a day.
You can also use ready-made preparations “Fitogastrol” (analgesic, choleretic effect), “Gastrofit” (gastritis with normal and low acidity).
Drug treatment
Drug treatment is aimed at regulating the secretion of hydrochloric acid, eliminating Helicobacter pylori infection, normalizing motility, and improving digestion in lymphoid gastritis.
| With low acidity | With increased acidity |
| Acidity replenishing drugs: Pepsidil - normalizes the acidity of gastric juice, contraindicated in hyperacid gastritis. Course duration is 2-3 weeks. | Acid-reducing drugs: Cimetidine, Ranitidine, Omeprazole, esomeprazole - reduce the synthesis of hydrochloric acid. Contraindicated in cases of low acidity. Duration of treatment is 2-4 weeks. |
| Drugs that increase the secretion of gastric juice: Nicotinic acid (improves blood supply), citric acid (donor of acidic valences). The course of treatment is 10-14 days. | Antacids – protecting the gastric mucosa from hydrochloric acid: Maalox, Phosphalugel, Vikalin – neutralization of hydrochloric acid, protection of the gastric epithelium. Course – 10-14 days. |
| Improving blood circulation in the coolant: Curantil – improves microcirculation. The course of therapy is 2 weeks. | Enveloping and astringent agents: De-nol - creating a protective film on the surface of ulcers and erosions. The course of therapy is 4-8 weeks. |
| Improving motor skills: antispasmodics - Duspatalin, Motilium – acceleration of gastric peristalsis. | Antibiotics when HP is detected: Clarithromycin, Amoxiclav, Metronidazole - are used in combination to eradicate (destruct) Helicobacter pylori. |
Treatment is prescribed by a doctor. For eradication, a triple (omeprazole + clarithromycin + amoxicillin) or quadruple treatment regimen (omeprazole + De-nol + amoxicillin + metronidazole) is used. The duration of eradication therapy is 7-14 days.
Physiotherapy
Physiotherapeutic procedures begin after acute inflammatory processes have reduced and pain has disappeared. Physiotherapy is carried out in inpatient and outpatient settings, in sanatorium and resort institutions.
Physiotherapy methods and goals:
- Pain syndrome – electrophoresis of novocaine, papaverine; diadynamic currents, SMT therapy.
- Restoration of the epithelium of the gastric mucosa - galvanization, ultra-high frequency electric field.
- Correction of low acidity – inductothermy.
- Correction of high acidity – electrosleep.
In the rehabilitation of patients with chronic lymphocytic gastritis, balneotherapy is recommended. Preference is given to hydrocarbonate-sodium, calcium-magnesium and carbon dioxide mineral waters with a low degree of mineralization (salt content less than 1 g/l) - these are the waters “Arshan”, “Rzhanskaya”, “Essentuki Novaya-55”, “Essentuki No. 20”. Table and medicinal table waters improve the regeneration of the gastric mucosa.
Requirements for the use of mineral waters are determined by the level of acidity:
- In case of high acidity, it is recommended to take mineral water at a temperature of 38-42 °C 60-90 minutes before meals at the rate of 3 ml/kg body weight - a course of up to 30 days.
- If acidity is preserved, take mineral water 40-60 minutes before meals, degassed (without gas) at a temperature of 38-45°C - course for up to 30 days.
- For gastritis with low acidity, water at a temperature of 38-42 ° C is prescribed 45-60 minutes before meals, 200-250 ml per day, it is recommended to drink slowly, through a straw - a course of up to 30 days.
Additionally, therapeutic baths are used: coniferous, radon, mineral.
Mud applications to the epigastric region relieve inflammation, normalize the motor function of the digestive tract, stimulate secretory function and increase the period of remission for gastritis.
Important! A set of physiotherapeutic procedures, taking into account their combined positive effect, is prescribed only by a physiotherapist. With concomitant uterine fibroids, polyps of the stomach and intestines, extrapulmonary tuberculosis and ulcerative colitis, physical therapy is contraindicated.
Material and methods
The prospective study included 73 patients with GC who underwent radical surgery (R0) at the Orenburg Regional Clinical Dispensary from January 2009 to July 2010. The average age of the patients was 61.2±9.3 years (from 34 to 78 years, median - 61 years old). There were 43 men (58.9%), 30 women (41.1%). The tumor was localized in the upper third in 14 (19.2%) patients, in the middle third in 18 (24.7%) and in the lower third in 41 (56.1%). The intestinal type of gastric cancer was noted in 41 (56.2%) patients and diffuse - in 32 (43.8%). Well-differentiated adenocarcinoma (G1) was observed in 27 (36.9%) patients, moderately differentiated (G2) - in 14 (19.3%), poorly differentiated adenocarcinoma and undifferentiated GC - in 9 (12.3%) and signet ring cell carcinoma ( RCC) - in 23 (31.5%). The distribution of patients by disease stage was as follows: T1-2N0M0 - in 34 (46.6%), T3N0M0 - in 9 (12.3%), T3-4N1M0 - in 9 (12.3%) and T3-4N2M0 - in 21 (28.6%) patients.
Subtotal proximal resection was performed in 10 (13.7%) patients, subtotal distal resection in 56 (76.7%) and gastrectomy in 7 (9.5%). Lymphadenectomy in the D2 volume was performed in all patients, with D3 elements in 38 (52.0%). In 7 (12.3%) patients, combined operations were performed: splenectomy was performed in 3 cases, transverse colon resection was performed in 2 cases, and cholecystectomy was performed in one case. The study did not include patients with decompensation of chronic diseases, acute infectious pathology, severe allergic processes, or those receiving corticosteroids, antihistamines, non-steroidal anti-inflammatory drugs, or neoadjuvant chemotherapy.
After removal of the drug, the stomach was opened along the greater curvature. A biopsy of the tumor and macroscopically unchanged coolant was performed, 3-5 cm from the proximal edge of the tumor. The tissue samples taken were placed in neutral formalin. The material was carried out according to standard methods and embedded in paraffin. Sections 4–5 μm thick were stained with hematoxylin and eosin and immunohistochemically using anti-CD20 antibodies (Epitope Specific Rabbit Antibody, Thermo Fisher Scientific) at a dilution of 1:400. The material for study by immunohistochemical (IHC) methods was fixed with 10% neutral formalin for 24 hours, embedded in paraffin, sections 4 μm thick were prepared, which were applied to highly adhesive glasses and dried at a temperature of 37 °C for 18 hours. Deparaffinization and unmasking of antigens were carried out in the RT module at a temperature of 121 °C for 20 minutes, followed by cooling for 60 minutes. The imaging system used was Ultra Vision LP Detection System HRP Polymer & DAB Plus Chromogen. As a negative control, sections were similarly incubated with antibody dilution solution (UltrAb Diluent). In the peritumoral area, the presence of focal lymphoid B-cell infiltrates and the number of lymphoid follicles (LF) in the coolant (none, single - no more than 2 in the field of view, multiple - more than 2 follicles in the field of view) were assessed using a semi-quantitative method. The presence of normal and atypical light centers in them was also assessed. The density of diffuse B lymphocytes was counted using a magnification of 400, over an area of 1200×1800 pixels, taken as a conventional unit of area (ARU), with a resolution of 10 pixels/cm (0.42×0.28 mm2). The metric grid density was 216 points.
Statistical processing of the study results was carried out using the Statistica 6.0 application package. B cell density was expressed as mean (M) ± standard deviation (σ). Comparison of indicators between groups was carried out using parametric and nonparametric methods (LSD and Mann-Whitney tests). The relationship between indicators was determined using nonparametric methods (Spearman rank correlation and gamma). The reliability of differences in the frequencies of signs in the studied groups was assessed using the χ2 test. Analysis of overall and disease-free 3-year survival was performed using the Kaplan-Meier method. Comparison of survival rates between groups of patients was carried out using the long-rank test. Differences between indicators were considered significant at p
<0,05.