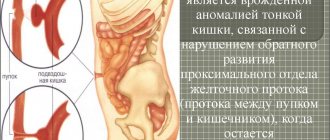
Causes of Hirschsprung's disease
Hirschsprung's disease is a congenital disease that develops in utero; scientists believe that one of the main etiological factors is the lack of nutrients in the mother's body during intrauterine development of the fetus. Due to a lack of necessary substances, during the development of innervation of the fetal digestive system, areas of the large intestine appear that do not have nerve endings; often specialists cannot determine the cause of this disease.
The length of the area with missing innervation can vary: from a few centimeters to the entire area of the large intestine. It is not uncommon for this pathology to be transmitted hereditarily; about 50% of patients suffering from Hirschsprung's disease have a history of close relatives with the same disease.
There is an assumption that dysfunction of the development of the intestinal nervous system is provoked by a mutation in the structure of DNA genes.
In newborn boys, this disease occurs 4-5 times more often than in girls.
Clinic
The main symptoms of Hirschsprung's disease are chronic constipation and lack of independent bowel movements. These symptoms usually occur immediately after the baby is born. Normally, the passage of the first stool (meconium) is observed during the first two days. Therefore, the first person who may suspect a disease is a pediatrician. According to the State Scientific Center of Coloproctology, the diagnosis is made in early childhood only in 19% of cases. Of these 19% of patients, two out of three children have an erased course of the disease (Achkasov S.I., Blagodarny L.A.)
Therefore, it is worth remembering about this disease for a coloproctologist if he sees an adult patient with complaints of prolonged and persistent constipation. The clinical picture of the disease can be very variable and have no obvious symptoms. As already noted, Hirschsprung's disease is a genetic mutation in several genes, each of which individually does not cause the disease (at least one has not yet been identified). Therefore, it is still rare, but it is possible to encounter a mature patient who is unaware of his genetic illness. Their constipation is periodic and unstable.
Abdominal distension can be detected on examination in most patients. There may not be bloating, since the large intestine has been in a compensated state for a long time. In more severe cases, the enlarged, fecal-filled sigmoid colon can be palpated.
Symptoms of Hirschsprung's disease
The intensity of symptoms depends on the severity of the disease (the extent of intestinal damage).
In most cases, the clinical manifestations of this disease are diagnosed in the first days of a child’s life, sometimes in adolescence or adolescence; in adulthood it is rarely detected.
In newborns, the main symptoms of Hirschsprung's disease are: lack of feces (meconium) in the first days of life, increased gas formation, vomiting (in some cases with bile), and there are also other dyspeptic disorders (diarrhea, constipation).
In older children, there may be an increase in abdominal volume, a predisposition to persistent constipation, the development of malabsorption syndrome and, as a result, retardation in growth and development. As a result of frequent loss of blood in feces, anemia may develop, infection may occur and enterocolitis may develop. In case of intestinal infection, hyperthermia, vomiting and diarrhea are observed. Severe intoxication promotes expansion of the colon.
In adults, Hirschsprung's disease is manifested by the absence of the urge to empty the rectum, spastic pain along the colon, bloating, and intoxication of the body caused by the toxicity of accumulated substances. Sometimes a clinical sign of Hirschsprung's disease is partial heterochromia - uneven coloring of areas of the iris.
X-ray picture
X-ray picture: with aganglionosis of the entire colon and with the spread of the aganglionic zone to the terminal part of the ileum, dilated loops of the small intestine are visible on a survey radiograph of the abdominal cavity of a newborn (performed in the direct and lateral projection of the child).
This indicates obstruction of the distal small or large intestine. In cases of aganglionosis of the entire colon, retrograde filling of all parts of the small intestine, duodenum and even the stomach is possible (Neal, Chandler et al., 1970). During irrigoscopy, the colon is of normal caliber, but its shortening and smoothing of contours and bends are determined. If there is an aganglionic zone only in the terminal ileum, then during irrigoscopy a narrowed area and expansion of the intestinal lumen proximal to this section are observed.
In the presence of a segmental lesion, when the narrowing zone is not radiologically determined, which is possible in newborns and infants, since the expansion of the intestinal lumen above the narrowing zone has not yet had time to develop, it is almost always possible to establish in these patients an excessive accumulation of contrast mass above the narrowing site (cit . according to N. L. Kush, 1970), slow passage of barium through the aganglionic sections (usually the rectum and sigmoid colon) and rapid filling of the proximal sections of the colon.
When filling the large and small intestines with barium, it is possible to identify “filling defects” due to coprolites.
Peristaltic activity of the aganglionic zone is completely absent. The retention of barium in the intestine after a contrast enema for a day suggests a diagnosis of “Hirschspruit's disease”, even if it is not possible to identify a spastic zone. In cases where there is a large amount of gas in the colon, a narrowed segment can be distinguished. In some cases, compacted, calcified meconium is detected on the x-ray.
In older children, examination of the chest cavity organs reveals a high location of the domes of the diaphragm and limitation of their mobility, an increase in the pulmonary hilar pattern, and a displacement of the cardiovascular shadow.
A plain abdominal radiograph shows large amounts of gas and horizontal fluid levels in the colon. Sometimes fecal stones can be seen against the background of gas.
With the slow introduction of barium, a narrowing of the aganglionic part of the colon is determined, expressed to varying degrees: the narrower and longer it is, the easier the x-ray diagnosis. The narrowed area, most often located in the rectosigmoid region, may have a jagged or even contour; the wall, as a rule, is rigid and does not peristalt. Behind the narrowed section there is a gradual, “funnel-shaped” transition into the expanded part of the colon.
In cases where the aganglionic zone has a relatively wide lumen, the degree of narrowing of the intestinal lumen is judged by comparing it with the dilated part of the colon. The diameter of the expanded part of the colon varies: from insignificant to 25 - 30 cm. There is no haustral segmentation in this section, peristalsis is very sluggish or absent. Characterized by a delay in bowel emptying from barium suspension due to the presence of narrowing of the intestinal lumen. The relief of the mucous membrane of the aperistaltic zone is rough and hyperplastic.
“X-ray diagnosis of diseases of the gastrointestinal tract in children”, D.N. Maksumov, E.I. Agafonova, B.N. Kalmykov
Diagnosis of Favalli-Hirschsprung disease In the differential diagnosis of Favalli-Hirschsprung disease, the method of rectal biopsy proposed by Swenson in 1955 is recommended. It is indicated in cases of discrepancy between the clinic of congenital aganglionosis of the colon and X-ray data, as well as the failure of conservative treatment (Yu. F. Isakov , 1965). The rectal biopsy method is simple, safe and indicated at any age (even in newborns). Fabric defect...
A special case (Patient G.A., 8 years old) Patient G.A., 8 years old, was admitted to the hospital pediatrics clinic on August 22, 1970 with a referral diagnosis of rheumatic heart disease, combined mitral heart disease. Upon receipt of a complaint of shortness of breath, pallor, weight loss. According to the father, the child was diagnosed with congenital heart disease at the age of four. He is observed in the clinic, from where he was referred for consultation to the thoracic surgery clinic, and then...
Examination of older children Examination of older children begins with a survey fluoroscopy of the chest and abdominal cavity. It is necessary to pay attention to the location and mobility of the domes of the diaphragm, the position of the heart, and the degree of expansion of the colon. During irrigoscopy, the radiologist’s task is to determine the localization and extent of the aganglionic zone, the degree of its narrowing and expansion of the overlying sections. Then the length of the sigmoid colon and its mobility are determined...
Etiology and pathogenesis There is no consensus on the etiology and pathogenesis of this disease, however, in recent years, thanks to the accumulated experience and histological examination data, great importance has been attached to the neurogenic theory. In 1901, Tittel first noted changes in the structure of the nodes of the Auerbach plexus in the intestinal wall in Hirschsprung's disease. I. A. Abrikosov (1909) believed that the basis of the disease is insufficient reflex...
Macroscopic data for Favalli-Hirschsprung disease Macroscopically, Favalli-Hirschsprung disease is characterized by narrowing of the distal part of the intestine, widening of the proximal part and a funnel-shaped transition between these parts. The muscle layer in the areas of narrowing and expansion is thickened, especially in the transition area, the mucous membrane is hypertrophied, and there is no haustral segmentation. If aganglionosis also covers the rectum, then it is hypoplastic and its lumen is narrowed. The extent of the lesion varies. YU….
Treatment of Hirschsprung's disease
The only correct treatment for Hirschsprung's disease is surgery. During surgery, the affected area of the colon is removed and the terminal section of the intestine is connected to its healthy section.
Basically, all stages of this operation are always carried out within one surgical intervention, but there are exceptions - the operation in such cases consists of two stages. At the first stage of the two-stage operation, resection (excision) of the affected area of the intestine and colostomy are performed (excision of the end of the healthy intestine through an incision in the abdomen). The stool is evacuated into a special container that the patient has to carry with him. After normalization of the patient’s intestinal function, the second stage of the operation begins - intestinal reconstruction, the task of which is to connect the free end of the healthy intestine with the rectum and close the colostomy (suturing the hole in the abdomen).
As a rule, after an operation to eliminate the affected areas of the intestine, patients gradually normalize the process of digestion and excretion of feces, that is, a complete recovery occurs. Sometimes patients may notice a tendency to constipation, but this problem can be eliminated with the help of laxatives.
Story
Danish pediatrician Harald Hirschsprung in 1888 described the case history of two children with a similar clinical picture: severe constipation and bloating. The children needed daily enemas. Despite the lack of any information about the nature of the disease, continuous therapy was carried out, but both children still died. A post-mortem examination was carried out. At autopsy, a narrowing of the rectum was discovered, and above the narrowed section there was a pronounced dilation of the intestinal loops with ulceration of the mucous membrane. And not only expansion, but also “the wall is also greatly hypertrophied, especially the muscle layer.” Hirschsprung was not the first to describe the disease (20 cases had been described before 1888), but he was the one to provide a detailed description of the disease based on his clinical experience.
The name “Hirschsprung's disease” itself became widely used only at the end of the 20th century. Until 1916, the doctor described 10 more cases of the disease.
Few diseases in pediatric surgery have generated as much controversy and confusion as the optimal treatment of Hirschsprung's disease.
Minimizing negative consequences
To minimize constipation, diarrhea and other undesirable effects after surgery, patients are recommended to adhere to a special diet, which is based on the consumption of foods rich in plant fiber.
The risks of postoperative complications include the development of enterocolitis due to intestinal infection, therefore, if there is an increase in body temperature, vomiting, diarrhea, or signs of intestinal bleeding, you should immediately consult a doctor.
In mild cases of Hirschsprung's disease, surgical interventions can be abandoned and symptomatic treatment can be performed using siphon enemas.
CONSERVATIVE TREATMENT
- Diet – about 60% of the diet of a person with problems with bowel movement should consist of vegetables and fruits. Products with a fixing effect, such as coffee, strong tea, chocolate, pears, and products made from refined white flour, are excluded. The diet should contain a sufficient amount of vegetable oils and fermented milk products. Drinking regimen at the rate of 30 ml of pure raw water per kilogram of body weight per day;
- Probiotics and prebiotics are drugs that improve the condition of the intestinal microbiota;
In severe forms of aganglionosis, surgery is recommended in infancy. - Vitamins B, C and A;
- Massage and gymnastics to improve peristalsis;
- Enemas - depending on the severity, simple or siphon;
- Candles. To empty the intestines, you can use locally irritating drugs, such as Microlax, Glycerin suppositories;
- Laxatives. They may work well for some forms of Hirschsprung's disease. The safest remedy is lactulose - Duphalac. You can also use Senade, Forlax, magnesia sulfate, vaseline oil.
Classification
Classification of Hirschsprung's disease according to A.I. Lenyushkin 1. Rectal 25% - With damage to the proximal part of the rectum - With damage to the ampullary and supramullary parts 2 Rectosigmoid 70% - With damage to the distal part of the rectum - With damage to most or all of the sigmoid colon 3. Subtotal 3% - With damage to the entire left half - With the spread of the process to the right half of the colon 4. Total - Damage to the entire colon - With spread to the ileum