Signs of liver cirrhosis, symptoms and treatments
Liver cirrhosis is a chronic disease accompanied by structural changes in the liver with the formation of scar tissue, shrinkage of the organ and a decrease in its functionality.
It can develop against the background of prolonged and systematic alcohol abuse, viral hepatitis with its subsequent transition to a chronic form, or as a result of autoimmune disorders, obstruction of the extrahepatic bile ducts, cholangitis.
Science knows of cases where this disease was caused by prolonged heart failure, parasitic liver lesions, hemochromatosis, etc.
Some historical data
Since ancient times, the liver has been considered as important an organ as the heart. According to the inhabitants of Mesopotamia, the liver produces blood and the soul lives. Hippocrates also described the connection between liver diseases and jaundice, as well as ascites. He argued that jaundice and hard liver were a bad combination of symptoms. This was the first judgment about liver cirrhosis and its symptoms.
Cirrhosis of the liver and its causes were described in 1793 by Matthew Baillie in his treatise Morbid Anatomy. In his work, he clearly linked the consumption of alcoholic beverages with the occurrence of symptoms of liver cirrhosis. In his opinion, middle-aged and older men were more likely to get sick. The British dubbed cirrhosis the “gin plague” or “gin liver.”
The term cirrhosis comes from the Greek “kirrhos”, which means yellow and belongs to René Théophile Hyacinthe Laennec, a French physician and anatomist. Many scientists have worked and continue to work on the study of liver cirrhosis to this day. Virchow, Kuehne, Botkin, Tatarinov, Abelov and others proposed many theories about what liver cirrhosis is, its symptoms, causes, methods of diagnosis and treatment.
Reasons for the development of cirrhosis
Among the main reasons leading to the development of the disease are:
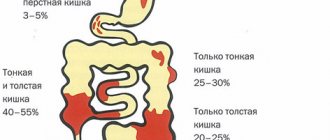
- Viral hepatitis, which, according to various estimates, leads to the formation of liver pathology in 10-24% of cases. The disease results in such types of hepatitis as , , D and the recently discovered hepatitis G;
- Various diseases of the biliary tract, including extrahepatic obstruction, cholelithiasis and primary sclerosing cholangitis;
- Disturbances in the functioning of the immune system. Many autoimmune diseases lead to the development of cirrhosis;
- Portal hypertension;
- Venous congestion in the liver or Budd-Chiari syndrome;
- Poisoning with chemicals that have a toxic effect on the body. Among such substances, industrial poisons, salts of heavy metals, aflatoxins and mushroom poisons are especially harmful to the liver;
- Diseases transmitted by inheritance, in particular, genetically determined metabolic disorders (anomalies of glycogen accumulation, Wilson-Konovalov disease, deficiency of α1-antitrypsin and galactose-1-phosphate-uridyltransferase);
- Long-term use of medications, including Iprazide, anabolic steroids, Isoniazid, androgens, Methyldopa, Inderal, Methotrexate and some others;
- Drinking large doses of alcohol for 10 years or more. There is no dependence on a specific type of drink; the fundamental factor is the presence of ethyl alcohol in it and its regular intake into the body;
- The rare Osler-Rendu disease can also cause cirrhosis.
In addition, it is worth mentioning separately about cryptogenic cirrhosis, the causes of which remain unclear. It occurs in the range from 12 to 40% of cases. Provoking factors for the formation of scar tissue can be systematic malnutrition, infectious diseases, syphilis (which can cause cirrhosis in newborns). The combined influence of etiological factors, for example, a combination of hepatitis and alcoholism, significantly increases the risk of developing the disease.
Classification
The modern classification of the disease in question is based on taking into account etiological, morphogenetic and morphological criteria, as well as clinical and functional criteria. Based on the reasons behind the influence of which cirrhosis of the liver developed, the following variants are determined:
- biliary cirrhosis (primary, secondary) (cholestasis, cholangitis);
- circulatory cirrhosis (arising against the background of chronic venous stagnation);
- metabolic and nutritional cirrhosis (lack of vitamins, proteins, accumulation cirrhosis resulting from hereditary metabolic disorders);
- infectious (viral) cirrhosis (hepatitis, biliary tract infections, parasitic liver diseases);
- toxic cirrhosis, toxic-allergic cirrhosis (food and industrial poisons, medications, allergens, alcohol);
- cryptogenic cirrhosis.
Depending on the clinical and functional characteristics, liver cirrhosis is characterized by a number of the following features:
- level of hepatic cell failure;
- general nature of the disease (progressive, stable or regressive);
- the degree of portal hypertension relevant to the disease (bleeding, ascites);
- general activity of the disease process (active cirrhosis, moderately active cirrhosis, as well as inactive cirrhosis).
Risk factors
The onset of the disease comes as a shock to some patients. But more often, cirrhosis of the liver develops against the background of a number of factors. The development of the disease can be triggered by the following diseases and conditions:
- alcoholic organ damage;
- viral hepatitis B, C, D;
- metabolic organ damage;
- vascular lesions of the liver;
- diseases of the biliary tract;
- drug lesions;
- cryptogenic cirrhosis.
Being at risk, the patient must be aware that untimely diagnosis, delay in treatment, or failure to follow the doctor’s recommendations will lead to a sharp progression of the disease. In the last stage, cirrhosis cannot be treated; transplantation is not allowed, since the body will reject the transplanted organ.
Treatment is carried out using different methods, and the successful identification of the cause of the disease also depends on the effectiveness.
In the early stages, patients at risk are examined. They take a general blood test, a coagulogram, a stool test for occult blood, and check markers of viral hepatitis. The creatinine level is checked, an ultrasound and a liver complex of biochemical studies are prescribed. Round-the-clock medical monitoring will improve the quality of life of patients in the last two stages.
Portal cirrhosis of the liver
The most common form of the disease, which is characterized by damage to liver tissue and death of hepatocytes. Changes occur due to poor nutrition and alcohol abuse. In 20%, portal cirrhosis can cause Botkin's disease. First, the patient complains of disorders of the digestive tract. Then external signs of the disease develop: yellowing of the skin, the appearance of spider veins on the face. The last stage is characterized by the development of ascites (abdominal dropsy).
Lifespan
Medical statistics are disappointing. The disease develops quickly and is often asymptomatic in the first stages. The last stages leave the patient no hope.
| Stages | Description | Deadlines |
| First | It is difficult to determine the presence of the disease on your own. Decreased performance, lethargy, mild pain on the right side, loss of appetite. | 6-7 years. |
| Second | Vomiting, nausea and frequent fever. Jaundice may develop, and the pain in the side intensifies. The urine darkens and the stool turns white. The development of accompanying syndromes is possible. | Up to 5 years. |
| Third | Against this background, carcinoma, thrombosis, and hepatic coma develop. Signs of the third stage include fever, vomiting, muscle atrophy, sepsis, and bleeding. | Up to 3 years. |
| Fourth | It is possible to develop ascites against the background of serious lesions. They die within six months. The liver is decomposing and deformed. Other internal organs are damaged. | Up to six months. |
From a medical point of view, the stages are called compensation, subcompensation, decompensation, terminal. The dates are indicated only if the doctor’s instructions are fully observed. If you continue bad habits and ignore recommendations, you can cut the term in half.
First signs
Early symptoms indicating cirrhosis include the following:
- A feeling of bitterness and dryness appears in the mouth, especially often in the morning;
- The patient loses some weight, becomes irritable, and gets tired faster;
- A person may be bothered by periodic stool disorders, increased flatulence;
- Periodically occurring pain localized in the right hypochondrium. They tend to increase after intense physical activity or after taking fatty and fried foods, alcoholic beverages;
- Some forms of the disease, for example, postnecrotic cirrhosis, manifest themselves in the form of jaundice already in the early stages of development.
In some cases, the disease manifests itself acutely and there are no early signs.
Symptoms of cirrhosis
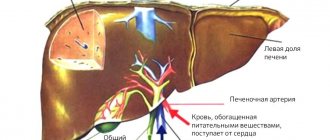
Cirrhosis is characterized by general symptoms: weakness, decreased ability to work, discomfort in the abdomen, dyspeptic disorders, increased body temperature, joint pain, flatulence, pain and a feeling of heaviness in the upper abdomen, weight loss, asthenia. Upon examination, an enlargement of the liver, compaction and deformation of its surface, and sharpening of the edge are revealed. At first, there is a uniform moderate increase in both lobes of the liver; later, as a rule, the increase in the left lobe predominates. Portal hypertension is manifested by a moderate enlargement of the spleen.
The detailed clinical picture is manifested by the syndromes of hepatic cell failure and portal hypertension. There is bloating, poor tolerance to fatty foods and alcohol, nausea, vomiting, diarrhea, a feeling of heaviness or abdominal pain (mainly in the right hypochondrium). In 70% of cases, hepatomegaly is detected, the liver is compacted, and the edge is sharpened. In 30% of patients, palpation reveals a nodular surface of the liver. Splenomegaly in 50% of patients.
Low-grade fever may be associated with the passage of intestinal bacterial pyrogens through the liver, which it is unable to neutralize. The fever is resistant to antibiotics and resolves only when liver function improves. There may also be external signs - palmar or plantar erythema, spider veins, scanty hair in the axillary and pubic area, white nails, gynecomastia in men due to hyperestrogenemia. In some cases, the fingers take on the appearance of “drum sticks.”
In the terminal stage of the disease, in 25% of cases there is a decrease in liver size. Jaundice, ascites, peripheral edema due to overhydration (primarily swelling of the legs), external venous collaterals (varicose veins of the esophagus, stomach, intestines) also occur. Bleeding from veins is often fatal. Hemorrhoidal bleeding occurs less frequently and is less intense.
The first signs in an adult
Asthenovegetative syndrome is the first sign of the development of the disease. The patient feels lethargic, tired, and unable to work. Reactions become weak, causeless irritability appears. Frequent headaches are added to the symptoms. Additionally, the following dyspeptic complex of syndromes is present:
- nausea;
- vomit;
- belching;
- abdominal pain;
- loss of appetite;
- heaviness in the stomach;
- bloating.
This includes constipation, diarrhea and their alternation. It is noteworthy that all symptoms can also occur with other ailments. In biliary cirrhosis, symptoms of biliary tract damage occur at the initial stage. The success of treatment is determined by the stage of the disease, gender and age of the patients. So in men the disease develops longer and more easily than in women.
In a fifth of all patients, it is impossible to identify the cause of cirrhosis. The first signs may be completely absent. Patients do not notice a deterioration in their quality of life and do not contact a medical specialist. The initial stage is characterized by minimally expressed symptoms, the clinical stage is accompanied by a typical picture of the course of the disease. The terminal stage is characterized by irreversible changes and leads to death.
First stage
Most patients are unaware of the development of pathology. The initial stage may be accompanied by pain, intestinal disorders, and lack of appetite. But more often it does not reveal itself. Pain in the abdominal cavity is localized in the right hypochondrium, in the side. The following conditions may exist:
- heaviness in the stomach after eating fatty foods;
- pain in the right side after drinking alcohol;
- bitter taste in the mouth after eating, after waking up;
- persistent dryness in the mouth and sinuses.
Abdominal ultrasound and laboratory tests are used for diagnosis. Timely diagnosis and effective treatment at the first stage provide a good prognosis. The main condition for prolonging life is compliance with medical recommendations. Often this entails a complete change in lifestyle and eating habits.
Decreased appetite and concentration indicate an inflammatory process in the liver.
At the first signs, you should contact a medical specialist. Most patients associate symptoms with increased physical activity, fatigue at work, and vitamin deficiency.
Second stage
The prognosis and stages of liver cirrhosis are of concern to patients who have just encountered the disease. People get acquainted with statistics and disappointing scenarios. But here it is important to consider the clinical picture of each patient individually.
Patients with the same stage can have dramatically different prognoses.
It can occur in women, men and even children (extremely rare). In the second stage, symptoms become more pronounced. The transition from the first degree to the second can take from six months to two years, depending on the patient’s lifestyle. Connective scar tissue grows, causing irreversible necrosis. Therapy involves taking medications that prevent the development of irreversible processes. The second stage is characterized by:
- yellowing of the skin;
- frequent nausea, vomiting;
- white feces;
- darkening of urine;
- loss of appetite;
- sharp pain in the right side.
Hypertension may develop. Severe pathology is treated with complex treatment. It is provoked by the formation of scar tissue nodes on the surface of the liver. Portal hypertension is treatable in the first two stages. Most often it simply stops.
Third stage
The disease is actively developing. Progression leads to liver failure. Vivid symptoms appear. During the period of decompensation, an optimistic prognosis of up to 15 years is possible if the patient does not have severe complications and strictly follows the doctor’s instructions and diet.
At the third stage, a liver transplant is required, otherwise life expectancy will not exceed 3 years.
The severe stage of progression of the disease is characterized by the inability to process artificial compounds. Tablets relieve pain, but do not cure the patient, but aggravate the situation. The stage is accompanied by the following symptoms:
- diarrhea;
- vomit;
- weight loss;
- lack of strength;
- atrophy of the arm muscles;
- heat.
Without monitoring by a specialist, the risk of death is high. It is necessary to perform an operation, then rebuild the patient’s regimen, introduce a diet and medications. If everything went well, the patient should be examined regularly. Typically, checks take place every three months in the first year after surgery, then every six months.
Fourth stage
It cannot be cured or undergoes compensatory treatment. Patients are left with a disappointing diagnosis and live for up to six months. There is no point in transplanting a liver; the drugs are ineffective. Against the backdrop of a severe course of the disease, a number of concomitant pathologies develop. The disease is accompanied by severe pain.
The terminal stage is characterized by liver deformation and organ decomposition.
The patient is in serious condition for the first weeks, then falls into a coma. Extensive liver deformation affects other organs. The spleen is distorted, putting pressure on tissues and organs. Developing:
- anemia;
- leukopenia;
- decrease in prothrombin.
The danger of the fourth stage is brain damage. In rare cases, life expectancy reaches six months. If the disease progresses intensively, the patient dies within three to four months. After entering a comatose state, the patient does not come out of it. If pathologies develop abruptly, the patient may die within two weeks.
The functioning of the circulatory and nervous systems is disrupted. The heart and lungs work with difficulty, and patients require artificial ventilation if they are severely affected. There is no treatment, only relief of a serious condition.
Consequences
Liver cirrhosis, in principle, alone does not cause death; its complications in the decompensation stage are deadly. Among them:
- Ascites in cirrhosis is an accumulation of fluid in the abdominal cavity. A diet with limited protein (up to 0.5 grams per kg of body weight) and salt, diuretics, and intravenous administration of albumin (a protein drug) are prescribed. If necessary, resort to paracentesis - removal of excess fluid from the abdominal cavity.
- Spontaneous bacterial peritonitis is inflammation of the peritoneum due to infection of the fluid in the abdominal cavity (ascites). Patients have a fever of up to 40 degrees, chills, and intense abdominal pain. Long-term broad-spectrum antibiotics are prescribed. Treatment is carried out in the intensive care unit.
- Hepatic encephalopathy. Manifests itself from minor neurological disorders (headache, increased fatigue, lethargy) to severe coma. Since it is associated with the accumulation of protein metabolism products (ammonia) in the blood, protein is limited or excluded from the diet, and a prebiotic is prescribed - lactulose. It has a laxative effect and the ability to bind and reduce the formation of ammonia in the intestines. For severe neurological disorders, treatment is carried out in the intensive care unit.
- Hepatorenal syndrome is the development of acute renal failure in patients with liver cirrhosis. Stop the use of diuretics and prescribe intravenous albumin. Treatment is carried out in the intensive care unit.
- Acute variceal bleeding. Arises from varicose veins of the esophagus and stomach. The patient becomes increasingly weak, blood pressure drops, pulse quickens, and vomiting appears mixed with blood (the color of coffee grounds). Treatment is carried out in the intensive care unit; if ineffective, surgical treatment methods are used. To stop bleeding, intravenous administration of octropide is used (to reduce pressure in the blood flow of the abdominal vessels), endoscopic treatment (ligation of varicose veins, sclerotherapy). Transfusion of solutions and blood components is carried out carefully to maintain the required level of hemoglobin.
- The development of hepatocellular carcinoma is a malignant neoplasm of the liver.
The definitive treatment for hepatocellular carcinoma and decompensated liver cirrhosis is liver transplantation. Replacing a patient's liver with a donor's liver.
Third degree cirrhosis life expectancy
With such a diagnosis, life expectancy depends on the disease and how it progresses. About half a percent of people with this stage 3 can live for three or four years . The survival rate may become much lower the following complications develop
- diaphragmatic hernia;
- when intra-abdominal pressure increases, hemorrhoids develop;
- hydrothorax;
- internal organs are displaced;
- esophageal reflux.
If you follow the therapy correctly , then you can increase the continuation of life by one or two years , but doctors are not able to do more, because the cells that are functioning are replaced by non-functioning fibrosis. If the patient does not have viral infections, it is possible to prolong his life by transplanting a new organ .
Complications in the third degree of cirrhosis, where life expectancy decreases:
- bleeding of the gastrointestinal tract;
- hepatocellular carcinoma, that is, the rapid development of a malignant tumor;
- with hepatopulmonary syndrome;
- hepatic gastropathy;
- hepatoridal syndrome: sluggish kidney function, large amounts of toxins in the blood, renal failure;
- hepatic encephalopathy (neuro-muscular spasms, unbalanced behavior, inadequate consciousness);
- Varicose veins: when the veins and esophagus and rectum dilate.
Diagnostics
Determining the diagnosis of liver cirrhosis takes place in several stages. The diagnosis itself is made on the basis of instrumental research data:
- Magnetic resonance or computed tomography is the most accurate diagnostic method.
- Biopsy is a method of histological examination of material taken from the liver, which makes it possible to establish the type of large- or small-nodular cirrhosis and the cause of the development of the disease.
- Ultrasound – as a screening. Allows you to establish only a preliminary diagnosis, but is indispensable when diagnosing ascites and portal hypertension.
If, upon diagnosis, histological examination does not allow determining the cause of the disease, the search for it continues. To do this, perform a blood test to determine the presence of:
- antimitochondrial antibodies;
- Hepatitis C virus RNA and hepatitis B virus DNA using the PCR method;
- alpha-fetoprotein – in order to exclude blood cancer;
- copper and cerruloplasmin levels;
- level of immunoglobulins A and G, level of T-lymphocytes.
At the next stage, the degree of damage to the body due to liver damage is determined. For this use:
- liver scintigraphy - radionuclide study to determine working liver cells;
- biochemical blood test to determine indicators such as sodium and potassium levels, coagulogram, cholesterol, alkaline phosphatase, total and fractional bilirubin, AST, ALT, lipidogram, proteinogram;
- degree of kidney damage – creatinine, urea.
Absence or presence of complications:
- Ultrasound to exclude ascites;
- eliminating internal bleeding in the digestive tract by examining stool for the presence of hidden blood;
- FEGDS - to exclude varicose veins of the stomach and esophagus;
- sigmoidoscopy to exclude varicose veins in the rectum.
In cirrhosis, the liver can be palpated through the anterior wall of the peritoneum. On palpation, the tuberosity and density of the organ are noticeable, but this is only possible at the stage of decompensation.
Ultrasound examination clearly identifies foci of fibrosis in the organ, and they are classified into small ones - less than 3 mm, and large ones - over 3 mm. With the alcoholic nature of cirrhosis, initially small nodes develop; a biopsy determines specific changes in liver cells and fatty hepatosis. In later stages of the disease, the nodes enlarge and become mixed, and fatty hepatosis disappears. Primary biliary cirrhosis is characterized by an enlarged liver while maintaining the structure of the biliary tract. In secondary biliary cirrhosis, the liver becomes enlarged due to obstructions in the bile ducts.
Overall percentage and statistics
In 70% of cases, cirrhosis actively develops against the background of hepatitis C. There are no primary symptoms, the disease occurs in a latent form. The patient may notice a slight discomfort, or may not notice the irreversible changes occurring in the body at all. Other causes of development may be the following ailments and conditions:
- toxic hepatitis;
- autoimmune hepatitis;
- fatty steatosis;
- heart failure.
Occurs against the background of alcohol dependence. Inflammatory processes and weakness, pain localized both in the right side and in the hypochondrium on the same side. To make an accurate diagnosis, it is necessary to do an ultrasound of the abdominal cavity and undergo laboratory tests. According to statistics, the disease of the third and fourth degrees cannot be cured.
The average duration of the disease varies from five to six years. If detected early, life expectancy increases to nine years. The course of the pathology is influenced by the stage of the disease, the age and gender of the patient, compliance with recommendations, the presence of complications or concomitant ailments.
Stages of liver cirrhosis
The course of the disease, as a rule, is characterized by its own duration, with the following main stages being distinguished:
- Compensation stage. It is characterized by the absence of symptoms of cirrhosis, which is explained by increased work of the remaining liver cells.
- Subcompensation stage. At this stage, the first signs of liver cirrhosis are noted (in the form of weakness and discomfort in the right hypochondrium, decreased appetite and weight loss). The functions inherent in the liver are performed in an incomplete manner, which occurs due to the gradual loss of resources of the remaining cells.
- Stage of decompensation. Here we are already talking about liver failure, manifested by severe conditions (jaundice, portal hypertension, coma).
Additional Information
The most common causes of death are self-medication, delaying going to the doctor, and non-compliance with medical recommendations.
Liver cirrhosis is a disease with rapid progression. The first stage is the longest and is asymptomatic. The worse the patient’s lifestyle, the faster the disease will move into the second stage. The intensity of symptoms increases gradually.
It is impossible to cure established cirrhosis.
For viral hepatitis, pegylated interferons are used. For biliary cirrhosis, medications are prescribed to narrow the bile ducts. For autoimmune lesions, safe immunosuppressants are selected. In case of severe damage, an organ transplant operation is performed.
The specialist determines the duration and method of treatment. If the outcome is successful, the patient must follow the recommendations and diet for the rest of his life. Otherwise, the forecast can be considered invalid. Life expectancy will decrease sharply.
How to treat liver cirrhosis?
In general, the treatment of liver cirrhosis is selected on a strictly individual basis - therapeutic tactics depend on the stage of development of the disease, the type of pathology, the general health of the patient, and concomitant diseases. But there are also general principles for prescribing treatment.
These include:
- The compensated stage of liver cirrhosis always begins with eliminating the cause of the pathology - in this case, the liver is still able to function normally.
- The patient needs to adhere to a strict diet - even a slight violation can trigger the progression of liver cirrhosis.
- It is impossible to carry out physiotherapy or heat treatment for the disease in question. Physical activity is also excluded.
- If the disease is at the stage of decompensation, the patient is placed in a medical institution. The fact is that with this course of the disease, the risk of developing severe complications is very high and only medical workers will be able to promptly pay attention to even a slight deterioration in the condition and prevent the development of complications that lead to the death of the patient.
- Most often, hepatoprotectors, beta-blockers, sodium and ursodeoxycholic acid preparations are prescribed for treatment.
General advice for patients with liver cirrhosis:
- Rest as soon as you feel tired.
- To improve digestion, patients are prescribed multienzyme drugs.
- Avoid heavy lifting (this may cause gastrointestinal bleeding)
- Measure your body weight and abdominal volume at the navel level daily (an increase in abdominal volume and body weight indicates fluid retention);
- If there is fluid retention in the body (edema, ascites), it is necessary to limit the intake of table salt to 0.5 g per day, liquid intake to 1000-1500 ml per day.
- To monitor the extent of damage to the nervous system, it is recommended to use a simple handwriting test: write a short phrase, for example, “Good morning,” in a special notebook every day. Show your notebook to your relatives - if your handwriting changes, contact your doctor.
- Every day, count the fluid balance for the day (diuresis): count the volume of all liquid taken orally (tea, coffee, water, soup, fruit, etc.) and count all the liquid released during urination. The amount of fluid released should be approximately 200-300 ml more than the amount of fluid taken.
- Aim for stool frequency 1-2 times a day. Patients with liver cirrhosis are recommended to take lactulose (Duphalac) to normalize intestinal function and the composition of the intestinal flora in favor of “good” bacteria. Duphalac is prescribed in a dose that causes soft, semi-formed stools 1-2 times a day. The dose ranges from 1-3 teaspoons to 1-3 tablespoons per day, selected individually. The drug has no contraindications; it can be taken even by small children and pregnant women.
Treatment of pathological manifestations and complications of cirrhosis means:
- Reducing ascites using conservative (diuretic drugs according to the regimen) and surgical (removal of fluid through drains) methods.
- Treatment of encephalopathy (nootropics, sorbents).
- Relief of manifestations of portal hypertension - from the use of non-selective beta-blockers (propranolol, nadolol) to ligation of dilated veins during surgery.
- Preventive antibiotic therapy to prevent infectious complications during planned visits to the dentist, before instrumental procedures.
- Treatment of dyspepsia through nutritional correction and the use of enzyme preparations without bile acids (pancreatin). In such cases, it is also possible to use eubiotics - bactisubtil, enterol, bifidumbacterin and lactobacterin.
- To relieve skin itching, antihistamines are used, as well as drugs containing ursodeoxycholic acid.
- Prescription of androgens for men with severe manifestations of hypogonadism and correction of the hormonal levels of women to prevent dysfunctional uterine bleeding - under the supervision of an endocrinologist.
- The use of drugs containing zinc is indicated for the prevention of cramps during normal muscle activity and in the complex treatment of liver failure to reduce hyperammonemia.
- Prevention of osteoporosis in patients with chronic cholestasis and primary biliary cirrhosis, in the presence of autoimmune hepatitis with the use of corticosteroids. To do this, calcium is additionally introduced in combination with vitamin D.
- Surgical correction of portal hypertension for the prevention of gastrointestinal bleeding includes the application of vascular anastomoses (mesentericocaval and splenorenal) as well as sclerotherapy of existing dilated veins.
- In the presence of single foci of degeneration into hepatocellular carcinoma and the severity of the disease of class A, patients are advised to undergo surgical removal of the affected liver segments. In case of clinical class B and C disease and massive lesions, while awaiting transplantation, antitumor treatment is prescribed to prevent progression. To do this, they use both the effects of currents and temperatures (percutaneous radiofrequency thermal ablation) and chemotherapy by targeted injection of oil solutions of cytostatics into the vessels supplying the corresponding segments of the liver (chemoembolization).
Treatment of such a serious and fatal complication as acute massive bleeding from the veins of the esophagus includes:
- Local application of a Blackmore probe, with the help of which an air cuff is inflated in the lumen of the esophagus, compresses the dilated bleeding veins.
- Targeted injection of the esophageal wall with sclerosing substances.
- Blood replacement therapy.
Unfortunately, this condition becomes the main cause of death in patients with cirrhosis of the liver.
How long do people live with cirrhosis with and without complications?
Liver cirrhosis rarely occurs without complications. Against the background of liver damage, the body's resistance to various ailments sharply decreases. Varicose veins of the esophagus, bleeding and pneumonia develop. The following pathologies often occur:
- Liver cancer
. A malignant tumor forms. Often provoked by hepatitis D and C. Rarely amenable to effective treatment. - Thrombosis
. Formation of blood clots in the portal vein system. Normal blood flow stops and the cells gradually die. - Hepatic coma
. Damage to the nervous system causes the liver to shrink in size. The patient falls into a stupor and after a while goes into a coma. If a coma occurs at the fourth stage, it leads to death. - Hepatorenal syndrome
. Kidney function is impaired due to alcohol abuse.
A dangerous disease is complicated by the presence of pathologies. The risk of death increases if complications are not recognized in time. Treatment of concomitant diseases is ineffective due to liver failure. With the progression of the pathologies described above, life expectancy is reduced to ten to twelve days. The specified period depends on how long the patient delayed diagnosis.
Diet for liver cirrhosis
Following a diet for liver cirrhosis involves, first of all, avoiding foods that have a high protein content. After all, in patients with liver cirrhosis, the digestion of protein foods is disrupted, and as a result, the intensity of putrefaction processes in the intestines increases. The diet for liver cirrhosis involves periodic fasting days, during which the patient does not eat food containing protein at all. In addition, an important point is to limit the use of table salt with the main meal.
The diet for liver cirrhosis involves the exclusion of all products that contain baking soda and baking powder. You should not eat pickles, bacon, ham, seafood, corned beef, canned food, sausage, sauces with salt, cheeses, or ice cream. To improve the taste of products, you can use spices and lemon juice instead of salt.
The diet for liver cirrhosis allows the consumption of small amounts of dietary meat - rabbit, veal, poultry. You can eat one egg once a day.
Disease prognosis
Cirrhosis of the liver is incurable unless a liver transplant is performed. With the help of the above drugs you can only maintain a more or less decent quality of life.
How long people with liver cirrhosis live depends on the cause of the disease, the stage at which it was discovered and the complications that had appeared at the time of treatment:
- with the development of ascites they live 3-5 years;
- if gastrointestinal bleeding develops for the first time, from 1/3 to half of people will survive it;
- if hepatic coma develops, this means almost 100% mortality.
There is also a scale that allows you to predict life expectancy. It takes into account test results and the degree of encephalopathy:
| Parameter | Points | ||
| 1 | 2 | 3 | |
| Ascites | No | The abdomen is soft, goes away under the influence of diuretics | The abdomen is tense, its volume does not decrease well when taking diuretics |
| Changes in personality, memory, sleepiness | No | Mild degree | Strongly expressed |
| Total bilirubin | Less than 34 µmol/l | 31-51 µmol/l | More than 51 µmol/l |
| Albumen | 3.5 g/l or more | 2.8-3.5 g/l | Less than 2.8 g/l |
| Prothrombin index | More than 60% | 40-60% | Less than 40% |
| Sum of points | 5-6 | 7-9 | 10-15 |
| How long do they live? | 15-20 years | It is necessary to transplant the liver, but postoperative mortality is 30% | 1-3 years. If a transplant is performed at this stage, the probability of dying after the operation is 82 out of 100 |
Factors influencing life expectancy
The number of years lived with problems with liver cirrhosis is influenced by a number of features relating to the patient’s daily diet and activity. If he has not accepted the rule that alcohol , then his life will be shorter than that of those who have decided to give up addiction forever.
Chronic infections and diseases of internal organs make themselves felt and gradually toxins from insufficient liver function accumulate in the body, aggravating the situation. Therefore, it is important to undergo a medical examination on time and identify illnesses in their early stages.
Compliance with a special diet prescribed by your treating specialist is the key to additional years , so proper nutrition and sufficient saturation with healthy drinks gives strength to fight the disease.
Another factor that directly affects life expectancy is the duration of such a diagnosis . The disease, which has been observed for decades, is difficult to treat and puts a strain on the entire body , reducing expectancy .
Prevention
Liver cirrhosis is a rather long-term process that can be stopped and treated. The main key to success is to go to the doctor on time. However, it is one of those diseases that can be easily avoided by following certain preventive measures, including:
- vaccination against hepatitis B in childhood;
- rational and proper nutrition;
- avoiding starvation and overeating;
- giving up alcohol and smoking to exclude alcoholic cirrhosis and toxic liver damage;
- annual ultrasound and endoscopic examination;
- timely seeking medical attention from a doctor;
- adequate intake of vitamin and mineral complexes;
- strict suppression and treatment of drug addiction.
Preventive measures to prevent viral hepatitis will also help avoid the development of cirrhosis.
Influencing factors
It is impossible to determine liver cirrhosis at home. The earlier the disease is detected, the more effective the treatment will be. The course of pathology is influenced by:
- the presence of concomitant pathologies;
- causes of liver damage;
- compliance with doctor's instructions;
- stage of illness;
- patient's gender;
- patient's age.
Life expectancy also depends on the factors described above. By giving up bad eating habits, smoking and drinking alcohol, a person with a strong immune system lives longer than indicated in the medical literature. Older patients die harder and faster than younger ones.
Women also get sick more severely than men and are less responsive to treatment. For women, effective treatment is possible only at the first stage, for men - at the first and second. The disease is provoked by a viral infection, alcohol intoxication, protein deficiency, and lack of vitamins. The method of treating the disease depends on the cause.