Peptic ulcer (stomach ulcer)
The main significance for the formation of gastric ulcer is an imbalance between the protective mechanisms of the mucous membrane and the influence of aggressive endogenous factors (concentrated hydrochloric acid, pepsin, bile acids) against the background of a disorder of the evacuation function of the gastrointestinal tract (gastric hypokinesia, duodenogastric reflux, etc.) . Inhibition of protection and slower recovery of the mucous membrane is possible against the background of atrophic gastritis, with chronic Helicobacter pylori infection, ischemia of stomach tissue against the background of collagenosis, long-term use of NSAIDs (the synthesis of prostaglandins slows down, which leads to a decrease in mucus production).
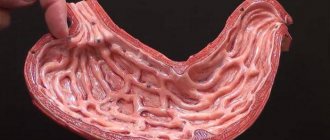
The morphological picture of gastric ulcer undergoes a number of changes. The primary substrate for the occurrence of ulcers is erosion - superficial damage to the gastric epithelium, which forms against the background of necrosis of the mucous membrane. Erosions are usually detected on the lesser curvature and in the pylorus of the stomach; these defects are rarely isolated. The size of erosions can range from 2 millimeters to several centimeters. Visually, erosion is a mucosal defect that does not differ in appearance from the surrounding tissues, the bottom of which is covered with fibrin. Complete epithelization of erosion with a favorable course of erosive gastritis occurs within 3 days without the formation of scar tissue. If the outcome is unfavorable, erosions transform into acute gastric ulcers.
An acute ulcer is formed when the pathological process spreads deep into the mucous membrane (beyond its muscular plate). The ulcers are usually single, take on a rounded shape, and look like a pyramid when cut. In appearance, the edges of the ulcer also do not differ from the surrounding tissues; the bottom is covered with fibrin deposits. Black coloration of the bottom of the ulcer is possible when the vessel is damaged and hematin is formed (a chemical substance formed during the oxidation of hemoglobin from destroyed red blood cells). A favorable outcome of an acute ulcer consists of scarring within two weeks; an unfavorable outcome is marked by the transition of the process to a chronic form.
The progression and intensification of inflammatory processes in the area of the ulcer leads to increased formation of scar tissue. Because of this, the bottom and edges of a chronic ulcer become dense and differ in color from the surrounding healthy tissue. A chronic ulcer tends to enlarge and deepen during an exacerbation; during remission it decreases in size.
Examination of work capacity and employment for gastric ulcers
One of the most important tasks of the attending physician is to determine the patient’s ability to work both for the period of treatment and for more distant periods of his life.
Patients with peptic ulcer disease in the acute phase should be considered temporarily disabled, regardless of the duration of the disease and the results of x-ray examination. In the presence of a recent fresh process, even if it is not pronounced and does not occur with pronounced clinical manifestations, bed rest in combination with antiulcer treatment is necessary (in a hospital setting, a sanatorium, or, in extreme cases, at home). The patient must be recognized as temporarily disabled, regardless of profession. The point of view existing among some doctors that in the initial period, as well as with successful outpatient treatment, one can limit oneself to this latter and, therefore, recognize the patient as able to work, should be considered incorrect. A number of observations indicate that the most persistent and long-term long-term effect occurs during treatment in a hospital, where there is always a sufficient amount of X-ray film and qualified laboratory assistants taking pictures. It should be emphasized once again that not only in the presence of a firmly established peptic ulcer, but also in the case of a reasonable suspicion of the latter, the patient should be recognized as temporarily disabled (especially in the initial period of the disease) and a course of antiulcer treatment should be simultaneously carried out. This event, in mandatory connection with subsequent preventive measures (om. prophylaxis), could significantly reduce the number of severely and long-term ill patients with peptic ulcer disease.
The issue of the ability to work and employment of patients with peptic ulcer disease is of great national importance. According to statistics, approximately from 6 to 12% of patients undergoing inpatient treatment (in surgical and therapeutic departments) are patients with peptic ulcer disease, mostly with a long period of illness. It should be noted that these statistics still do not reflect the true state of affairs, since not all patients with peptic ulcer disease are treated in a hospital.
In addition to establishing the temporary disability of patients with peptic ulcer disease, attending physicians must determine the ability to work of these patients for longer periods. We are talking about the examination of work ability and the most rational employment of patients with peptic ulcer disease in order to prevent relapses, progression of the disease and prevent possible complications.
In this regard, it is necessary to dwell on the issue and the role of the professional factor as an etiological factor in the development of peptic ulcer disease. It should be emphasized that so far it has not been possible to reliably establish the significance of any occupational factor as an etiological factor in the occurrence of peptic ulcer disease. Some authors attached importance to lead intoxication. However, when comparing different professional jobs, it turned out that people working with lead suffer from peptic ulcers no more often than people in other professions. There is no doubt that occupational factors, as well as work and nutritional regimens associated with the profession and the nature of work, play a significant role in the occurrence of relapses or exacerbations of peptic ulcer disease.
Numerous clinical and outpatient observations (E.M. Erman) indicate the importance for the development of peptic ulcers in professions that require predominantly nervous and physical stress, especially severe, as well as professions that interfere with maintaining a proper diet (work in different shifts, frequent business trips, traveling and so on.). In addition to these moments, which provoke relapses or exacerbation of the disease, work in conditions of unfavorable forced body position, frequent bending, long walking and body concussions apparently plays a negative role (E. M. Erman, F. I. Karamyshev, etc.) .
There are also indications of the importance of high temperature in the room, leading to a violation of the drinking regime (hot workshops), the influence of high-frequency currents that can cause a disorder of the nervous system, as well as the possibility of the influence of certain toxic substances in production conditions. Particular attention should be paid to - poisons acting on the central and autonomic nervous system - tetraethyl lead, ethyl liquid, ethyl bromide, ethyl chloride, gasoline and some others. However, the question of what role they play in the occurrence of peptic ulcer disease and its course is subject to special study.
When assessing the ability to work of patients with peptic ulcer disease, it is necessary to take into account the characteristics of the clinical course of the disease and, depending on this, recommend one or another type of employment, including a number of organizational measures in this direction. Working capacity is associated to a large extent with the stage of the disease, and the latter depends, firstly, on the anatomical and functional changes of the affected organ, and secondly, on the compensatory reactions of the body as a whole, the degree of which is significantly dependent on the state of the central nervous system. Ability to work is also determined by social factors, i.e., the requirements of the profession and the patient’s work orientation.
Similar articles:
X-ray mammography
Ultrasound during pregnancy - pros and cons
BCG - Vaccine against tuberculosis
Examination by a gynecologist. What does it represent? How to make an appointment?
Medical furniture: types, purpose, characteristics
Crimea is a land of resorts and health resorts
Supply of medical equipment to Crimea
Features of medical translation
Erosive lesions of the stomach and duodenum
Erosive damage to the mucous membrane of the stomach and duodenum is one of the most frequently detected pathologies of the gastroduodenal zone. This is a superficial defect in the mucous membrane of the stomach and duodenum, which does not penetrate the muscle layer and heals without scar formation. It is found in 2-15% of patients undergoing endoscopic examination. Erosion was first described by Morgagni in 1756. However, the opportunity to study erosions in detail appeared only after the introduction of endoscopic diagnostic methods into gastroenterological practice.Currently, interest in the problem of erosive lesions of the mucous membrane of the stomach and duodenum has increased significantly. This is primarily due to the prevalence of this disease mainly among people of working age. Severe, often profuse bleeding, the source of which was erosion, has been described; often the source of bleeding is erosion, even in patients with concomitant ulcerative process. The possibility of malignancy of erosions cannot be excluded, and in some cases they serve as a morphological manifestation of the cancer process.
Etiology and pathogenesis.
In most cases, a violation of the integrity of the mucous membrane is a consequence of a violation of the normally existing balance between the factors of aggression and defense. This thesis also applies to erosive lesions.
Erosive damage occurs as a result of stressful circumstances (surgeries, injuries, burns, shock, psycho-emotional disorders). Erosion often occurs in people who abuse hot, rough, spicy food, coffee, and smokers. They complicate the course of various diseases (liver, kidneys, pancreas, heart, lungs, etc.), especially when they are decompensated. Thus, congestion in the portal vein with cirrhosis of the liver, thrombosis of the portal vein, chronic liver failure lead to the formation of erosions in the stomach and duodenum. Superficial defects of the mucosa often occur with a pronounced degree of diabetic ketoacidosis, diseases of the cardiovascular system and respiratory organs, leading to hypoxemia of organs and tissues, including the mucous membrane of the gastroduodenal zone. Erosion is not uncommon in patients with acute and chronic renal failure, pancreatitis, and malignant neoplasms. One of the main etiological factors of erosive lesions is duodenogastric reflux, which contributes to the detergent effect of bile on the gastric mucosa.
The appearance of erosions is often associated with the intake of alcohol and medications (corticosteroids, potassium chloride, rauwolfia preparations, salicylates, some antibiotics and other anti-inflammatory drugs), with exposure to the mucous membrane of corrosive substances (acids, alkalis, salts of heavy metals, etc.) .
The question of the role of Helicobacter pylori in the occurrence of gastric erosions, whose aggressive effect on the mucous membrane has been objectively proven, is controversial. The frequency of detection of Helicobacter pylori in biopsies of the mucous membrane depends on the nature of the pathological process and, according to some data, ranges from 15 to 94.4% in patients with erosions. Studies have also shown that such patients often have antibodies to Helicobacter pylori, as well as sensitization of lymphocytes to the antigens of these bacteria.
Acid-peptic aggression is also considered an important factor in the formation of chronic erosions. However, in recent years, scientists have tended to believe that a high level of gastric acidity turns into a damaging factor only when the protective ability of the mucous membrane decreases. At the level of cell population kinetics, these factors are manifested by a change in the balance between cell formation and cell death. Consequently, an erosive defect in the mucous membrane can occur even with normal or increased proliferation, if the processes of cell rejection increase to a greater extent.
To identify other, perhaps more significant etiological factors in the formation of erosions, attempts were made to study concomitant disorders in the body's immune system. In particular, using enzyme immunoassay, antibodies to pentagastrin were detected, which, being a biologically active pentapeptide of gastrin, has a secretory, motor and trophic effect on the digestive tract. There is evidence that, in addition to pentagastrin, the antibodies themselves are capable of binding various forms of endogenous gastrin, creating the preconditions for deterioration of the trophism of the mucous membrane.
Increasingly, works are appearing on the pathogenetic role of impaired prostaglandin metabolism in the occurrence of erosions of the gastroduodenal mucosa. In particular, it is assumed that the decrease in the content of prostaglandins in the area of the erosive defect is due to the blocking of the key enzyme of prostaglandin biosynthesis, cyclooxygenase, by lipoperoxides.
Classification.
Currently, there is no consensus on the systematization of existing data on erosive lesions of the gastrointestinal mucosa. There are several classifications of erosions, which in most cases are based on the endoscopic picture.
The most common is the classification proposed by V. Vodolagin (1996). According to this classification, a distinction is made between primary erosive defects, which are an independent pathology, and secondary ones, accompanying the underlying disease (severe damage to the liver, kidneys, cardiovascular system, etc.). In addition, erosions are distinguished as a manifestation of a malignant or systemic process in the gastric mucosa (malignant erosions in cancer, lymphoma, Crohn's disease, etc.). Benign erosions are divided into acute (hemorrhagic), chronic single and multiple, chronic erosive (lymphocytic) gastritis, as well as erosive-hemorrhagic gastritis and duodenitis. Acute (superficial, flat, hemorrhagic, “incomplete”) erosions are superficial defects of various shapes and sizes, covered with blood, hemorrhagic and fibrinous plaque against the background of altered or unchanged mucosa. They are often multiple and localized mainly in the body and subcardial part of the stomach. Acute erosions epithelialize quickly (usually within 2-14 days), without leaving any significant (macroscopic) traces; sometimes in their place an area of mucosal hyperemia may remain. The main distinguishing feature for chronic (“complete”, elevated, varioliform) erosions is the presence of a polypoid formation with a diameter of 3-8 mm, at the top of which there is a section of eroded mucous membrane with an umbilical depression in its center. The bottom of the defect is made of fibrin or hydrochloric acid hematin and a thin unstable layer of granulation tissue. Around such erosions there are hyperplastic, elongated and convoluted gastric pits.
Chronic erosions are characterized by the presence of a highly prismatic, intensively mucus-producing epithelium of the marginal zone. At the same time, a network of subepithelial vessels is developed, and there is an elongation of the cervical parts of the gastric glands. The muscular plate is intact or hyperplastic. In the zone of chronic erosion, there is an alternation of large areas of fibrosis, cystic expansion of the gastric glands, solitary follicles and intense mixed polymorphic cellular infiltration of the mucous membrane.
Chronic erosions exist for a long time (from 4 weeks to several years). Based on the nature of histological changes, this type of erosion can also be divided into “mature” and “immature”. In the first case, chronic erosion is epithelialized, and the swelling of the mucous membrane remaining in its place completely disappears; in the second case, the bulging remains due to developed tissue fibrosis and pronounced productive inflammation.
Clinic
It was believed that the clinical picture of erosive lesions corresponds to that of peptic ulcer disease and does not differ in specificity. However, if a peptic ulcer is accompanied by erosion, then the pain syndrome is particularly intense and persistent; in some patients it cannot be stopped even with treatment for 1.5-2 months. The exacerbation is more protracted than in patients with only a peptic ulcer. Very often, the erosive process occurs under the guise of the disease against which it developed (chronic cholecystitis, gastritis, etc.). In some cases, damage to the gastroduodenal mucosa by erosions may be asymptomatic.
All complaints presented by patients with erosive lesions of the gastroduodenal mucosa can be reduced to the following main syndromes: ulcer-like, in which the pain syndrome is clearly associated with food intake, night, “hungry” pain often occurs, dyskinesia develops early, and the healing time is relatively extended ; dyspeptic; without specific symptoms from the stomach and duodenum; hemorrhagic (clinically manifested by anemia and a positive reaction to occult blood in the stool). In some cases, in patients with peptic ulcer disease, the next exacerbation with a characteristic clinical picture is accompanied by the absence of a peptic ulcer, but there is hyperemia, swelling and erosion of the mucous membrane. Therefore, erosions should be regarded as a manifestation of disease activity.
The clinical course of the disease in the case of “complete” erosions has some features. The symptoms are scant: often heartburn, belching of air; rarely moderately severe fasting and early pain in the epigastric region after eating. Most chronic erosions generally proceed latently.
Diagnostics
The leading method for diagnosing erosions of the gastroduodenal mucosa is the endoscopic method. It makes it possible to distinguish two main types of erosion (see section “Classification”). Erosion of the stomach must be differentiated from the erosive-ulcerative form of cancer; for this purpose, a biopsy is necessarily performed, followed by a morphological assessment. Studies aimed at detecting Helicobacter pylori using a urease test or other methods are also advisable. Undoubtedly, the examination plan should include general clinical research methods: a general blood test (with hemorrhagic syndrome, iron deficiency anemia develops with characteristic laboratory signs); stool test for occult blood (for occult bleeding, the reaction is positive). Changes in gastric secretion parameters with erosive lesions are not pathognomonic.
Differential diagnosis of erosive lesions should be made with functional non-ulcer dyspepsia, chronic gastritis and duodenitis, peptic ulcer, and stomach cancer.
Treatment
Patients with erosions, as well as patients with peptic ulcers, require long-term treatment and subsequent endoscopic monitoring. In most cases, traditional antiulcer therapy is carried out (diet therapy, antibacterial therapy when HP is detected, the use of H2 blockers and proton pump inhibitors). But such therapy does not always give the desired result. In some cases, erosions continue to exist after the ulcer has healed, and sometimes previously undetected ones appear after the end of epithelization of the ulcer. All this indicates that the presence of erosions in the stomach or duodenum, especially in combination with edema and hyperemia of the mucous membrane, requires continued treatment, even if the ulcer has healed. Erosion in peptic ulcer disease should be considered a serious complicating factor; in this case, long-term therapy with individual selection of antiulcer drugs is indicated.
In case of secondary erosions, the drugs of choice are cytoprotectors: venter (sucralfate) 1 g 4 times a day, de-nol 120 mg 4 times a day and synthetic analogues of prostaglandins (cytotec 200 mg 3 times a day) for 4-8 weeks The possibility of accelerating the time of epithelization by local action on the erosive defect of the mucous membrane looks very attractive. The beneficial stimulating effect of low-intensity laser radiation on the processes of microcirculation, regeneration and immunomodulatory metabolism of the mucous membrane has been established. Treatment of hemorrhagic syndrome should be carried out in a surgical hospital.
Forecast.
Chronic erosions, unlike acute ones, can exist for a long time (weeks, months, in some cases even years). Their outcome may be the appearance of focal hyperplasia followed by the development of hyperplastic polyps. The possibility of malignancy of this type of erosion cannot be excluded.
Professor Igor MAEV. Ekaterina LEBEDEVA, Candidate of Medical Sciences. Moscow State Medical and Dental University.
Symptoms of the disease
The leading symptom of exacerbation of peptic ulcer is pain in the epigastric region, which can radiate to the left half of the chest and left shoulder blade, thoracic or lumbar spine.
Pain occurs immediately after eating (with ulcers of the cardial and subcardial parts of the stomach), half an hour to an hour after eating (with ulcers of the body of the stomach). With ulcers of the pyloric canal and duodenal bulb, late pain is usually observed (2-3 hours after eating), “hunger” pain that occurs on an empty stomach and goes away after eating, as well as night pain. It is typical that the pain goes away after taking antisecretory and antacid drugs.
With an exacerbation of a peptic ulcer, sour belching, nausea, constipation, and vomiting of acidic gastric contents, which brings relief, are also common. Typical for peptic ulcer disease are seasonal (spring and autumn) periods of increased pain and accompanying symptoms.