Study of nursing care technologies for pancreatitis
Observation of a patient with pancreatitis being treated in the surgical department of the Valuyskaya Central District Hospital made it possible to study the organization and technology of nursing care for this pathology.
On February 1, 2021, A.A. Ivanov was admitted to the therapeutic department of the Valuyskaya Central District Hospital. 46 years old with complaints of persistent pain in the epigastrium, aggravated by lying on the back, bloating, flatulence, nausea, vomiting that does not bring relief, pasty, shiny, profuse stools, weakness, lack of appetite. The pain appeared after eating fatty foods and alcohol.
During the first stage of the nursing process, an anamnesis was collected and a nursing examination was performed.
From the anamnesis it was found that in 2021, after a blunt abdominal injury, a splenectomy was performed for a splenic rupture. In the postoperative period, acute pancreatitis developed. Since 2021, the pain has become almost constant, due to the fact that the patient did not strictly follow dietary recommendations (excluding fat and limiting meat foods, categorical non-consumption of alcoholic beverages), after which a diagnosis of chronic pancreatitis was established. During 2021, he was hospitalized twice for relapse of chronic pancreatitis.
A physical examination revealed decreased nutrition, decreased skin turgor and moisture, and pale skin with a dirty gray tint. On palpation, pain in the epigastrium is determined; palpation of the abdomen is accompanied by pain radiating to the back, left hypochondrium, and shoulder girdle. The patient is agitated and worries about separation from loved ones.
At stage II of the nursing process, when forming a nursing diagnosis, we identified the patient's problems.
1. The patient's real problems:
1) priority:
- acute pain in the epigastrium and left hypochondrium due to inflammation of the pancreas, nausea due to intoxication, uncontrollable vomiting;
- secondary problems - lack of appetite due to pain in the epigastric region, psycho-emotional discomfort due to separation from loved ones, decreased performance due to hospitalization, decreased motor activity due to weakness.
2) potential problems:
- the risk of developing acute liver failure, pulmonary failure, secondary infection (purulent pancreatitis, sepsis, pancreatic fistulas), development of peritonitis, pancreatic necrosis, death.
At stage 3 of the nursing process, the correct formulation of the nursing diagnosis allowed the setting of goals.
Short-term goal: pain relief within 3 days. nausea, vomiting. Long-term goal: by the time of discharge, the patient will have no pain, bowel movements will normalize, and no complications will develop.
After setting goals, a nursing care plan was outlined with motivation for each action.
At stage IV, planned nursing interventions were implemented aimed at achieving the set goals.
Specific actions of the nurse to care for the patient in the first days after the patient’s admission to the hospital are aimed at alleviating the condition, ensuring rest for the pancreas, and relieving pain.
1. Creation of a therapeutic and protective regime (bed rest for 3 days) to reduce stress and relieve pain.
2. To relieve pain, dyspeptic disorders, manifestations of exocrine and intrasecretory pancreatic insufficiency:
- cold on the epigastric region, fasting for 3 days, then diet No. 5;
- in drinking mode, mineral or heated water, or rosehip decoction.
3. Drug treatment as prescribed by a doctor - to eliminate the clinical symptoms of the disease.
Cefazolin (1.0 g. Dissolve in 200 ml of 0.9% sodium chloride solution, IV slowly).
Contrical (10,000 units dissolved in 200 ml of 0.9% sodium chloride solution, IV slowly).
Papaverine (2% 2 ml, in ampoules IM 2 ml, 1 time per day).
Famotidine (0.8, 1 tablet 2 times a day).
Venter (1.0, 1 tablet 3 times a day).
4. Clinical and laboratory examination as prescribed by a doctor: OAM, OAC, blood test for residual nitrogen, urine test for diastase, ECG, ultrasound of the abdominal organs.
Independent nursing interventions were performed to ensure treatment effectiveness.
1. Monitoring compliance with bed rest, giving a comfortable position.
2. Creating conditions for good sleep,
3. Psycho – emotional peace. It is important to monitor the patient’s psychological state and, if possible, protect him from worries and worries. Patients do not always respond correctly to doctor’s recommendations; this is due to a lack of information about the disease. This is why conversation with the patient during the treatment process is so important. It is good if he finds out all the details of his disease and how unpleasant the consequences will be in cases of refusal of certain methods of prevention and treatment.
4. Assistance in performing hygiene procedures.
5. Monitoring the patient’s condition (skin, pulse, blood pressure, position in bed, breathing, physiological functions).
6. Timely implementation of medical prescriptions.
7. Teaching the patient diet therapy, monitoring diet compliance, talking with the patient about the role of diet in the treatment of acute pancreatitis. Nursing care for pancreatitis is not only about monitoring the composition of foods, but also ensuring that they are properly prepared. Hot food, food from the refrigerator and large portions are contraindicated. Food must meet all the requirements for such patients. This is one of the main components of the treatment process.
8. Conversation with the patient about the harmful effects of alcohol on the pancreas and maintaining a healthy lifestyle.
Stage V of the nursing process - assessing the effectiveness of nursing care.
On the 2nd day of treatment, vomiting stopped, and on the 4th day of treatment, the pain stopped. By the time of discharge, the symptoms of the disease had stopped, and the patient’s well-being had improved. The goal has been achieved.
Upon discharge, the patient was given nursing advice.
1. The physical activity regimen should be dosed. Physical exercise and sports activities should be limited in the first month after treatment.
2. Continued adherence to the diet. Meals should be frequent (5 - 6 times a day) .
Meals should not be plentiful - you need to take food in small portions. In order to prevent irritation of the gastric mucosa, products should be consumed in pureed form. Meals are prepared based on the principle of “mechanical sparing” of the digestive organs. Food should be consumed exclusively warm. It is preferable to boil or steam the products. It is necessary to increase the consumption of foods containing proteins (fish, meat, cottage cheese), reduce the consumption of carbohydrates (sugar, honey, sweets), and reduce the consumption of fatty foods. Products that have an increased juice-containing effect (cabbage broth, fish and meat broths) should be excluded from the diet. If acute pain occurs, a 1-2 day therapeutic fast is necessary.
3. Careful self-monitoring of the condition is necessary: taking medications, self-massage. In the process of treating patients with acute pancreatitis, special attention is paid to the use of antispasmodics and analgesics, the action of which is aimed at relieving spasms of the intestinal muscles. During attacks of chronic and acute pancreatitis, medications are used to relieve pain.
4. Giving up bad habits.
Thus, during the treatment process, the patient promptly fulfilled all doctor’s orders, followed the diet and department regimen. He followed all the nurse’s recommendations and actively asked questions that interested him, which contributed to the effectiveness of the therapy. During the treatment process, the patient was trained in the basic principles of diet therapy, which is fundamental in the treatment of pancreatitis. Conversations were held about complications and risk factors, which helped to increase awareness of this disease. The patient was motivated to maintain a healthy lifestyle and diet.
Conclusion
Analysis of medical literature and the results of our own research allowed us to draw the following conclusions…………….
Thus, the hypothesis that identifying risk factors and knowledge of nursing care technologies for pancreatitis helps to increase the effectiveness of treatment and prevent complications has been proven.
Bibliography
1. Aripov, U.A. Once again about cholelithiasis and its complications [Text]/ U.A. Aripov // J. Medical Journal. – 2014. No. 1. P. 13-15.
2. Bagnenko, S. F. Guide to emergency medical care [Text] / S. F. Bagnenko, A. G. Miroshnichenko, A. L. Vertkin, M. Sh. Khubutia. - M.: GEOTAR-Media, 2010. - 816 p.
3. Baranovsky, A.Yu. Dietetics. [Text]/: manual: 3rd ed. - St. Petersburg: Peter-Yug publishing house, 2008. - 1024 p.
4. Belousov, A. S. Diagnosis, differential diagnosis and treatment of diseases of the digestive organs [Text] / A.S. Belousov, V.D. Vodolagin, V.P. Zhakov. - M.: Medicine, 2002. - 424 p.
5. Belousov, S.S. Gastroesophageal reflux disease and duodenogastric reflux [Text] / S.S. Belousov, S.V. Muratov, A.M. Ahmad. - Nizhny Novgorod: NGMA, 2005. - 119 p.
6. Diseases of the pancreas: practical work. manual [Text]/ I.V. Maev, Yu.A. Curly. - M.: GEOTAR-Media, 2009. - 730 p.
7. Bratus, V.D. Acute gastric bleeding (differential diagnosis and treatment) [Text] / V.D. I'm brotherly. — 272 p.
8. Vakkasov, M.Kh. Diagnosis and treatment of chronic pancreatitis [Text]/ M.Kh. Vakkasov // Central Asian Medical Journal. — 2014. No. 2. P. 121-124.
9. Valenkevich, L. N. Diseases of the digestive organs. Guide to gastroenterology for doctors [Text]/ L.N. Valenkevich, O.I. Yakhontova. - M.: DEAN, 2006. - 656 p.
10. Introduction to gastroenterology [Text]: textbook. allowance / E.S. Ryss. - M.: SpetsLit, 2015. - 175 p.
11. Internal diseases [Text]: [textbook. for honey universities]: in 2 volumes / R. A. Abdulkhakov, V. G. Avdeev, V. A. Almazov and others; edited by N. A. Mukhina and others - 2nd ed., revised. and additional – T. 1. – Moscow: GEOTAR-Media, 2012. – 324 p.
12. Galimzyanov, F.V. Stages of application of minimally invasive technologies in the treatment of severe forms of pancreatitis [Text]/ F.V. Galimzyanov // In the materials of the IX conference of hepatological surgeons of Russia and the CIS countries. Saint Petersburg. - 2012. - No. 1- P. 194.
13. Gastroenterology and hepatology: diagnosis and treatment [Text]: a guide for doctors / ed. A.V. Kalinina, A.I. Khazanova; Ch. military wedge. hospital named after N.N. Burdenko. – M.: Miklos, 2007. – 600 p.
14. Gastroenterology [Text]: national guide / ed. V.T. Ivashkina, T.L. Lapina. – M.: GEOTAR-Media, 2008. – 700 p.
15. Gastroenterology [Text]: clinical recommendations] / ed. V. T. Ivashkina. 2nd ed. corr. and additional - M.: GEOTAR-Media, 2009. - 124 p.
16. Gastroenterology [Text]: reference. pract. doctor / A.V. Kalinin, I.V. Maev, S.I. Rapoport; under general ed. S.I. Rapoport. – M.: Medpress-inform, 2009. – 312 p.
17. Grigorieva, I.N. Alcoholic pancreatitis [Text]/ I.N. Grigorieva // Gastroenterology. — Consilium medicum application. - 2011. - P. 43 - 45.
18. Gubergrits, N.B. Pain in chronic pancreatitis: clinical and morphological comparisons [Text]/ N.B. Gubergrits // Ros. magazine gastroenterol., hepatol., coloproctol. - 2015.- pp. 58-66.
19. Gurvich, M.M. Diet for diseases of the digestive system [Text]/ M. Gurvich. – M.: GEOTAR – Media, 2006. – 288 p.
20. Ivashkin, V.T. Propaedeutics of internal diseases [Text]: workshop / V.T. Ivashkin, V.K. Sultanov. - St. Petersburg: Peter, 2000. - 384 p.
21. Ivashkin, V.T. Diarrhea syndrome [Text]/ V.T. Ivashkin, A.A. Sheptulin. – 2nd ed., expanded. and processed – M.: GEOTAR-MED, 2002. – 168 p.
22. Ivashkin, V.T. Nutrition for diseases of the digestive system [Text]/ V.T. Ivashkin, V.P. Shevchenko. – M.: GEOTAR-Media, 2005. – 351s
23. Kalinin A.V. Chronic pancreatitis: etiology, classification, clinical picture, diagnosis, treatment and prevention [Text]: textbook / A.V. Kalinin. - M.: TsIUV MO RF, 2012. - 44 p.
24. Clinical recommendations. Gastroenterology [Text]/ ed. V.T. Ivashkina. - M.: GEOTAR-Media, 2008. - 182 p.
25. Komarov, I.F. Internal diseases [Text]/ I.F. Komarov, V.G. Kukes, A.S.Smetnev.M.: “Medicine”, 1990. - 28 - 30 p.
26. Kubyshkin, V.A. Prevention and treatment of chronic pancreatitis [Text]/ V.A. Kubyshkin // Rus. honey. magazine - 2012. - P. 17 - 22.
27. Kucheryavyi, Yu.A. Patient with chronic pancreatitis: management errors, possible causes and solutions [Text]/ Yu.A. Curly // Gastroenterology. — Consilium medicum application. - 2014. - P. 46 - 55.
28. Kucheryavyi, Yu.A. Modern approaches to the diagnosis and treatment of chronic pancreatitis [Text]/ Yu.A. Curly // Diseases of the digestive system. - 2014.- pp. 18 – 24.
29. Maev, I.V. Chronic pancreatitis [Text]/ I.V. Maev, A.N. Kazyulin, Yu.A. Curly. – M.: Medicine, 2015. – 504 p.
30. Mayev, I.V. Theories and hypotheses of the pathogenesis of chronic pancreatitis [Text]/ I.V. Maev // Clinical perspectives of gastroenterology, hepatology. - 2015. - pp. 18 - 26.
31. Minushkin, O.N. Pancreatic diseases. Etiological aspects of the treatment of chronic pancreatitis [Text]/ O.N Minushkin // Consilium medicum. - 2015. - P. 27 - 32.
32. Minushkin, O.N. Chronic pancreatitis: some aspects of pathogenesis, diagnosis and treatment [Text]/ O.N Minushkin // Consilium medicum. - 2012. - P. 23 - 26.
33. Minushkin. HE. Modern principles and algorithms for the treatment of chronic pancreatitis [Text]/ O.N Minushkin // Materia Medica. — 2013. -S. 22 - 26.
34. Minushkin, O.N. Chronic pancreatitis [Text]/ O.N. Minushkin // Kremlin medicine. Clinical Bulletin. - 2014. - pp. 24 - 29.
35. Visual gastroenterology [Text]/ S. Keshav; lane from English S.V. Demicheva; edited by V.T. Ivashkina. – M.: GEOTAR-Media, 2005. – 135 p.
36. Parakhonsky, A.P. Relationship between psychological and somatic disorders in gastroenterological pathology [Text]/ A.P. Parakhonsky // Fundamental research. - 2007. - No. 2 - P. 93-93.
37. Polushkina, N.N. Diagnostic reference book for a gastroenterologist [Text]/ N.N. Polushkina. – M.: AST, 2007. – 671 p.
38. Rational pharmacotherapy of diseases of the digestive system: compendium / ed. V.T. Ivashkina, T.L. Lapina. – M.: Litterra, 2006. – 550 p.
39. Roitberg, G.E. Internal illnesses. Digestive system [Text]: textbook. allowance / G.E. Roitberg, A.V. Strutynsky. - M.: Medpress-inform, 2007. - 556 p.
40. Skripnichenko, D.F. Emergency abdominal surgery [Text] / D.F. Skripnichenko. M: 2008. - 90 - 93 p.
41. Zimmerman, Ya.S. Clinical gastroenterology [Text] / Ya.S. Zimmerman. – M.: GEOTAR-Media, 2009. – 413 p.
42. Shifrin, O.S. Clinical features of chronic pancreatitis in elderly patients [Text] / O.S. Shifrin // RZHGGK. - 2011. - No. 3. — P.35 — 40.
43. Filimonov, R.M. Gastroduodenal pathology and problems of restorative treatment [Text] / R.M. Filimonov. – M.: MIA, 2005. – 391 p.
44. Yakovenko, A.V. Chronic pancreatitis, clinical picture and diagnosis [Text]/ A.V. Yakovenko // Practicing doctor. – 2013 No. 13. — P. 34 — 35.
45. Yakovenko, A.V. Treatment of chronic pancreatitis [Text]/ A.V. Yakovenko // Practicing doctor. – 2013 No. 13.- P. 36 - 37.
acute pancreatitis
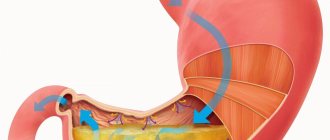
Category: Nursing in surgery/Injuries and diseases of the abdominal organsAcute pancreatitis is a peculiar pathological process that includes edema, inflammation, hemorrhagic infiltration and necrosis of pancreatic tissue
.
In the development of acute inflammation of the pancreas, according to the most common theory, the main factor is cell damage by prematurely activated enzymes. Under normal conditions, digestive enzymes are produced by the pancreas in an inactive form and are activated in the digestive tract. Under the influence of external and internal pathological factors, the production mechanism is disrupted, enzymes are activated in the pancreas and begin to digest its tissue. The result is inflammation, tissue edema develops, and the vessels of the gland parenchyma are affected.
Clinical picture
Acute pain, girdling in nature, is localized in the right and left hypochondrium, epigastric (epigastric) region. The pain radiates (radiates) to the left side of the body: to the shoulder, shoulder blade, lower ribs from the back. Intense pain, constant, even with drug treatment can continue for another day. The cause of pain is necrosis (death) of the tissue and nerve endings of the pancreas. Lack of appetite, aversion to food develops, is the result of a lack of excretion of pancreatic enzymes into the intestines. Nausea and vomiting caused by eating are the result of a lack of enzymes in the intestines necessary for normal digestion. Uncontrollable, profuse vomiting of stomach contents or bile, which does not bring relief. On examination, the skin is pale with a dark tint. Acute pancreatitis is characterized by specific symptoms of cyanosis, developing as a result of a sharp disruption of microcirculation, due to a decrease in the volume of circulating blood, as a result of profuse vomiting. Bluish spots form on different parts of the body (in the face and neck, sides of the abdomen, navel area).
Diagnostics
Gastroenterologists diagnose pancreatitis on the basis of complaints, physical examination, and identification of characteristic symptoms. When measuring blood pressure and pulse, hypotension and tachycardia are often noted. Laboratory tests of blood and urine, MSCT and ultrasound of the abdominal organs, and MRI of the pancreas are used to confirm the diagnosis.
Treatment
In case of acute pancreatitis, hospitalization is indicated. All patients were prescribed bed rest. The main goals of therapy are to relieve pain, reduce the load on the pancreas, and stimulate its self-healing mechanisms.
Therapeutic measures:
- novocaine blockade and antispasmodics to relieve severe pain;
- hunger, ice on the area of gland projection (creating local hypothermia to reduce its functional activity), parenteral nutrition, gastric contents are aspirated, antacids and proton pump inhibitors are prescribed;
- deactivators of pancreatic enzymes (proteolysis inhibitors);
- deactivators of pancreatic enzymes (proteolysis inhibitors);
- necessary correction of homeostasis (water-electrolyte, acid-base, protein balance) using infusion of saline and protein solutions;
- detoxification therapy;
- antibiotic therapy (broad-spectrum drugs in large dosages) as a prevention of infectious complications.
Patient care for acute pancreatitis
When caring for a patient, it is necessary to create peace for him, put him in a warm bed in the Fowler position, surround him with attention and good care
.
To create rest for the pancreas, the following measures are performed: a thin probe is inserted into the stomach and gastric and duodenal contents are removed, the stomach is washed with cold alkaline water, an ice pack is placed on the area of the pancreas, neither food nor water can be taken through the mouth - absolute hunger during 4-5 days, and sometimes more. After the hunger ends, you are allowed to drink alkaline mineral water, then weak tea.
The next day - diet No. 1, and only after 4-8 days the patient can be allowed to eat diet No. 2 and No. 5 .
See injuries and diseases of the abdominal organs
Saenko I. A.
Sources:
- Barykina N.V. Nursing in surgery: textbook. allowance/N. V. Barykina, V. G. Zaryanskaya.- Ed. 14th. - Rostov n/d: Phoenix, 2013.
- Private surgery: textbook. allowance/N. V. Barykina; under general ed. B.V. Kabarukhina. - Rostov n/d: Phoenix, 2008.